Procedure 39 Pollicization for Congenital Thumb Hypoplasia
 See Video 32: Pollicization
See Video 32: PollicizationIndications


Examination/Imaging
Clinical Examination
 The Blauth classification of thumb hypoplasia is useful in determining treatment options. Types IV (floating thumb) (Fig. 39-1) and V (absent thumb) (Fig. 39-2) are straightforward to identify clinically. However, it can be challenging to differentiate type IIIA (stable carpometacarpal [CMC] joint) from type IIIB (unstable CMC joint), and the trapezium and trapezoid are ossified only at 5 to 6 years of age, making radiographs less useful in decision making.
The Blauth classification of thumb hypoplasia is useful in determining treatment options. Types IV (floating thumb) (Fig. 39-1) and V (absent thumb) (Fig. 39-2) are straightforward to identify clinically. However, it can be challenging to differentiate type IIIA (stable carpometacarpal [CMC] joint) from type IIIB (unstable CMC joint), and the trapezium and trapezoid are ossified only at 5 to 6 years of age, making radiographs less useful in decision making.





Imaging
 Radiographs of the hands, wrists, and forearms are useful in determining the degree of metacarpal and phalangeal hypoplasia of the thumb and index finger. They can also identify other associated upper extremity anomalies, such as radial deficiency.
Radiographs of the hands, wrists, and forearms are useful in determining the degree of metacarpal and phalangeal hypoplasia of the thumb and index finger. They can also identify other associated upper extremity anomalies, such as radial deficiency.
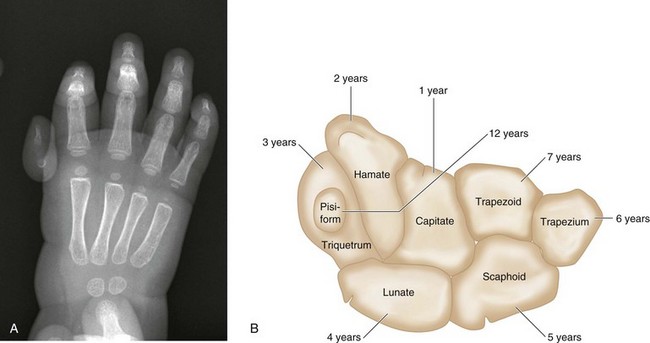
 The number of carpal bones seen on the radiograph gives a rough estimate of the age of the child (Fig. 39-3A). The order of ossification of carpal bones is detailed in Figure 39-3B. About one center appears per year from the age of 1 year to 7 years.
The number of carpal bones seen on the radiograph gives a rough estimate of the age of the child (Fig. 39-3A). The order of ossification of carpal bones is detailed in Figure 39-3B. About one center appears per year from the age of 1 year to 7 years.
 The presence of a tapered metacarpal without a base confirms type IIIB hypoplasia. Type IIIA hypoplasia is associated with full length of the metacarpal (Fig. 39-4).
The presence of a tapered metacarpal without a base confirms type IIIB hypoplasia. Type IIIA hypoplasia is associated with full length of the metacarpal (Fig. 39-4).

Surgical Anatomy
 After pollicization, the common digital artery to the index and long fingers is the primary blood supply to the transposed digit. The radial digital artery to the index finger may be absent, but the ability to perform index pollicization is not contingent on the presence of the radial digital artery when the main blood supply comes from the ulnar digital artery.
After pollicization, the common digital artery to the index and long fingers is the primary blood supply to the transposed digit. The radial digital artery to the index finger may be absent, but the ability to perform index pollicization is not contingent on the presence of the radial digital artery when the main blood supply comes from the ulnar digital artery.
Positioning


Exposures
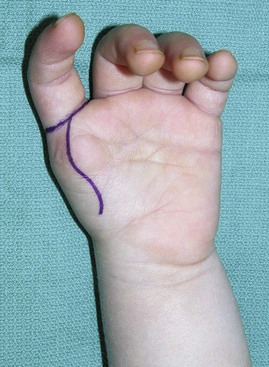
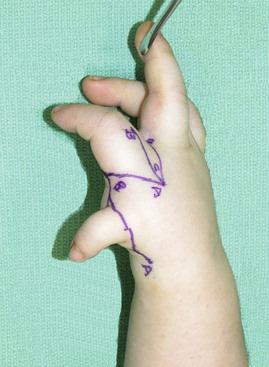
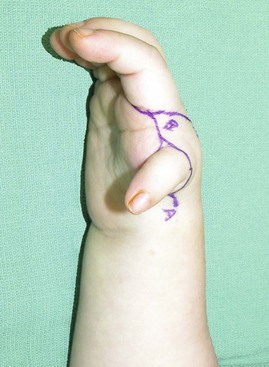
 A longitudinal curvilinear incision is marked over the palmar aspect of the index finger metacarpal (Fig. 39-5). A V-shaped incision is marked over the dorsum of the index finger metacarpal such that the apex is at the level of the neck of the metacarpal (Figs. 39-6 and 39-7). The dorsal and palmar incisions are connected at the base of the finger. A longitudinal incision is marked over the dorsum of the proximal phalanx, extending from the proximal interphalangeal (PIP) joint to the apex of the V.
A longitudinal curvilinear incision is marked over the palmar aspect of the index finger metacarpal (Fig. 39-5). A V-shaped incision is marked over the dorsum of the index finger metacarpal such that the apex is at the level of the neck of the metacarpal (Figs. 39-6 and 39-7). The dorsal and palmar incisions are connected at the base of the finger. A longitudinal incision is marked over the dorsum of the proximal phalanx, extending from the proximal interphalangeal (PIP) joint to the apex of the V.


Pearls
If the thumb is present, the hypoplastic digit may be filleted and the skin incorporated into the design of the skin flaps or into the first web space for additional soft tissue coverage (Figs. 39-8 and 39-9).
Procedure
Step 1
 The palmar skin incisions are made first, and thick skin flaps are raised.
The palmar skin incisions are made first, and thick skin flaps are raised.
Related posts:
 28: Pronator Teres Rerouting
28: Pronator Teres Rerouting
 33: Correction of Swan-Neck Deformity in the Rheumatoid Hand
33: Correction of Swan-Neck Deformity in the Rheumatoid Hand
 89: Total Wrist Fusion
89: Total Wrist Fusion
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


