Procedure 36 Syndactyly Release
 See Video 29: Syndactyly Release and Skin Grafting
See Video 29: Syndactyly Release and Skin Grafting
See Video 30: Syndactyly Release with Pentagonal Flap
Indications



Examination/Imaging
Clinical Examination
 Syndactyly is classified by the extent of fusion and the elements that are fused. Complete syndactyly involves the entire length of the fingers from the web to the tip (Fig. 36-1), whereas incomplete does not involve the entire length (Fig. 36-2). Simple syndactyly involves fusion of the skin only. Complex syndactyly describes fusion of the phalanges, usually the distal phalanx. Complicated syndactyly refers to fusion of multiple digits and is typically associated with other congenital anomalies such as Apert or Poland syndrome (Fig. 36-3).
Syndactyly is classified by the extent of fusion and the elements that are fused. Complete syndactyly involves the entire length of the fingers from the web to the tip (Fig. 36-1), whereas incomplete does not involve the entire length (Fig. 36-2). Simple syndactyly involves fusion of the skin only. Complex syndactyly describes fusion of the phalanges, usually the distal phalanx. Complicated syndactyly refers to fusion of multiple digits and is typically associated with other congenital anomalies such as Apert or Poland syndrome (Fig. 36-3).






Surgical Anatomy
 The web space is U shaped, with a 45-degree slope from the metacarpal head to the midproximal phalanx (Fig. 36-6). The web space of the index and long finger is at the same level, whereas the web space of the fourth web is more proximal (Fig. 36-7).
The web space is U shaped, with a 45-degree slope from the metacarpal head to the midproximal phalanx (Fig. 36-6). The web space of the index and long finger is at the same level, whereas the web space of the fourth web is more proximal (Fig. 36-7).



General Principles



Procedure
Release of Simple Complete Syndactyly
Exposures
 A proximally based dorsal rectangular flap for web reconstruction, along with interdigitating flaps, is used.
A proximally based dorsal rectangular flap for web reconstruction, along with interdigitating flaps, is used.
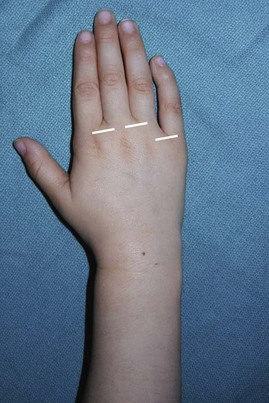
 The proximally based dorsal rectangular flap is designed by marking the metacarpal heads and a point on each digit at the midpoint of the proximal phalanx. The points are connected to form a proximally based flap with its base at the level of the metacarpal heads (Fig. 36-8).
The proximally based dorsal rectangular flap is designed by marking the metacarpal heads and a point on each digit at the midpoint of the proximal phalanx. The points are connected to form a proximally based flap with its base at the level of the metacarpal heads (Fig. 36-8).
 The interdigitating flaps are designed as two Zs, one on the dorsum and the other on the palmar surface, such that they form mirror images. The dorsal Z is designed first and connects the following four points sequentially (Fig. 36-9):
The interdigitating flaps are designed as two Zs, one on the dorsum and the other on the palmar surface, such that they form mirror images. The dorsal Z is designed first and connects the following four points sequentially (Fig. 36-9):
 For the flaps to interdigitate, the tips of the palmar and dorsal Zs must oppose each other. A 25-gauge needle is inserted through the skin from the dorsum to the palmar surface at the same level as the tip of the proximal dorsal flap (point B), and a palmar flap is designed such that the tip is on the other finger (Fig. 36-10A
For the flaps to interdigitate, the tips of the palmar and dorsal Zs must oppose each other. A 25-gauge needle is inserted through the skin from the dorsum to the palmar surface at the same level as the tip of the proximal dorsal flap (point B), and a palmar flap is designed such that the tip is on the other finger (Fig. 36-10A
Related posts:
 28: Pronator Teres Rerouting
28: Pronator Teres Rerouting
 33: Correction of Swan-Neck Deformity in the Rheumatoid Hand
33: Correction of Swan-Neck Deformity in the Rheumatoid Hand
 89: Total Wrist Fusion
89: Total Wrist Fusion
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


