Fig. 1
(a, b) AP (a) & lateral (b) clinical view of the leg; note the proximal half pin cluster pulled out of the bone and “shifted” medially during her fall the night before surgery; note the adherent scar at the medial ankle (arrow)
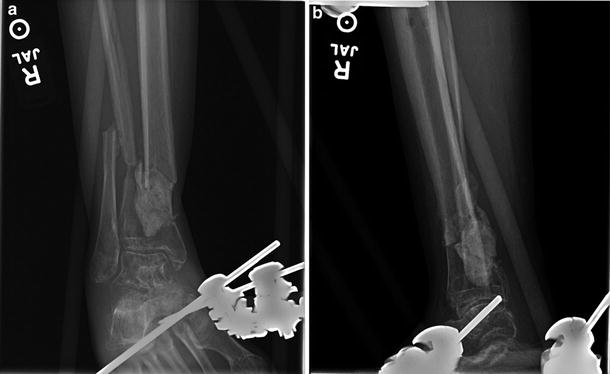
Fig. 2
(a, b) mortise (a) and lateral (b) X-ray view of the ankle; note the cement spacer and amount of tibial bone loss and shortening evident by the overlapping fibula
3 Preoperative Problem List
Open segmental distal tibial fracture
Tibia bone loss
Short peri-articular segment
Cement spacer
Compromised soft tissue
Need for approximately 6–7 cm of distal shortening & proximal lengthening
Avoid ankle equinus with bone transport
Avoid toe contractures
4 Treatment Strategy
For a multitude of reasons, I did not think internal fixation was the best option for this patient. Because of the segmental bone loss , short periarticular fragment, and compromised soft tissues, I opted for a circulator fixator.
My plan was to autograft and acutely shorten the periarticular region as much as the soft tissues would allow. This would require removing a segment of fibula. In the post-operative period, I would then use the fixator to slowly compress and dock the diaphysis into the peri-articular segment as the soft tissues allowed. I chose this method rather than preserving length and doing a pure bone transport because the leg was already shortened, and I wanted to dock the plafond segment as soon as possible after the autograft. I wanted to avoid reopening the compromised soft tissues for docking-site bone graft once it was closed.
Concurrent with the distal frame, I built a proximal lengthening frame and performed a metaphyseal tibia osteoplasty. To afford additional stability to the periarticular region and to stabilize the ankle during shortening and subsequent transport, I placed a static Ilizarov spanning the ankle joint. I worried about toe contractures during lengthening, so I initially pinned all five toes and attached these to the foot ring. I anticipated plafond union prior to proximal lengthening and consolidation. I planned to stage toe pin and foot frame removal at this time. I used TSF rings proximally and distally so that I could correct any residual angular deformity of the peri-articular block and proximal lengthening sites.
5 Basic Principles
I chose circular external fixation because of the compromised soft tissue envelope and the amount of bone loss distally. The fixator allowed concurrent proximal lengthening and distal compression and allowed stabilization of the foot and ankle. I acutely distracted several millimeters across the ankle and subtalar joints prior to stabilizing the static foot ring.
Proximal bone transport pulls the gastrocsoleus distally. Combined with significant distal shortening, I was concerned about ankle and toe contractures. Accordingly, I pinned the toes and spanned the ankle joint in neutral position. Attaching the circular ring at the plafond to the foot ring with threaded rods served to greatly increase the short plafond segment stability by creating a larger lever arm.
6 Images During Treatment
See Figs. 3, 4, 5, 6, and 7.

 8: Femoral Bone Defect
8: Femoral Bone Defect
 11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
 22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
 78: Two-Stage Treatment of a Chronic Foot Dislocation
78: Two-Stage Treatment of a Chronic Foot Dislocation
 84: Lapidus Fusion with External Fixation
84: Lapidus Fusion with External Fixation
 65: Closed Correction of Club Foot with Ilizarov
65: Closed Correction of Club Foot with Ilizarov




Related posts:
8: Femoral Bone Defect
11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
78: Two-Stage Treatment of a Chronic Foot Dislocation
84: Lapidus Fusion with External Fixation
65: Closed Correction of Club Foot with Ilizarov
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
