Fig. 1
(a) The anterior-posterior (AP) X-ray reveals that the joint surface has a complex fracture pattern which extends to the distal shaft. The fibular fracture overlap (arrows) heralds the amount of limb shortening and articular impaction. (b) The lateral X-ray provides information on the fracture fragments. The anterior fragment is actually aligned at anatomic length and the dome of the talus is impacted proximally. The posterior fragment has a complex fracture pattern (arrow) in which the joint fragment is impacted and disassociated from the posterior cortex. This will require an open reduction, disimpaction of the articular surface, and rotation of the fragment to recreate a congruent articular surface
3 Preoperative Problem List
1.
The injury will have rapid swelling which will compromise the safety of open operative approaches. Delayed open reduction and internal fixation after restoration of limb alignment with external fixation allow for soft tissue resuscitation. The typical delay is usually 10–21 days.
2.
The fracture is in a shortened position. A resuscitation bridging half pin distraction frame needs to be applied to the fracture. The distraction frame should accomplish four parameters: (1) The fracture is distracted to length or slightly over-distracted. (2) The dome of the talus is centered under the tibial plafond; it should be aligned axially on the AP and lateral flouroscopic images. (3) The foot is in correct rotation – the second toe is aligned with the tibia tubercle and patella. (4) The foot is in plantar neutral alignment – an equinus position is unacceptable.
3.
Check for compartment syndromes of leg and foot. These are rare complications but can occur.
4.
The pilon, like most articular injuries, has a complex fracture pattern that is not amenable to percutaneous reduction techniques. It will require an open approach.
5.
Further fracture information is needed for pre-operative planning. A CT scan is obtained after the joint spanning resuscitation external fixator is placed. CT scans done in a splint before fixator placement have little value.
See Figs. 2 and 3.

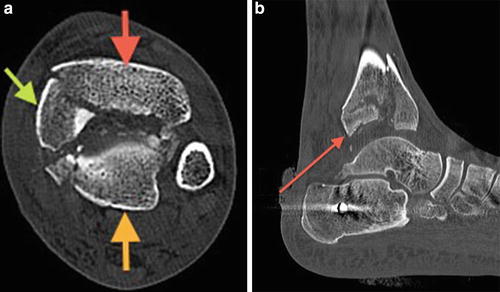
Fig. 2
Mortise view X-ray of the ankle after placement of a distraction external fixator. The fracture is distracted to length with the talus aligned axially with the tibial shaft. The fibula is still shortened because the flexible soft tissue attachment to the ankle and fracturing of the anterolateral fragment (arrow) do not provide enough stiffness to gain full length with traction. The calcaneal traction pin may be replaced with one or two tensioned wires to reduce the size of the tuberosity defect
Fig. 3
(a) Axial CT scan image at the level of the tibial plafond. This pilon fracture has a classic pattern. There is an anterior fragment (red arrow), a posterior fragment (orange arrow), and the medial malleolar fragment (green arrow) with edge comminution of the fragments and debris in the fracture gap. The fracture pattern also indicates that an anterior medial approach will provide the optimal exposure of the fracture. (b) Saggital image through mid-joint. The posterior fragment’s marginal impaction and comminution are clearly illustrated by the CT scan (arrow). The joint osteochondral fragment will need to have reduction onto the talar joint surface with bone graft placed to support it proximally. Of note, the transfixation calcaneal pin is placed too anterior. It should be placed more posterior and inferior in the calcaneal tubercle. This provides better bone purchase and avoids the medial neurovascular bundle
4 Treatment Strategy
Related posts:
 8: Femoral Bone Defect
8: Femoral Bone Defect
 11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
 22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
 78: Two-Stage Treatment of a Chronic Foot Dislocation
78: Two-Stage Treatment of a Chronic Foot Dislocation
 84: Lapidus Fusion with External Fixation
84: Lapidus Fusion with External Fixation
 65: Closed Correction of Club Foot with Ilizarov
65: Closed Correction of Club Foot with Ilizarov
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


