Procedure 3 Nail Bed Repair
Indications
 Open nail bed laceration (Fig. 3-1)
Open nail bed laceration (Fig. 3-1)
 Closed nail bed laceration with subungual hematoma involving greater than 50% of nail (Fig. 3-2)
Closed nail bed laceration with subungual hematoma involving greater than 50% of nail (Fig. 3-2)
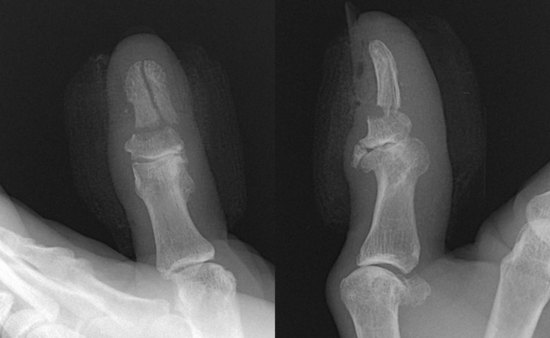
 Closed nail bed laceration with displaced distal phalangeal fracture
Closed nail bed laceration with displaced distal phalangeal fracture


Examination/Imaging
Clinical Examination
 Complete sensory examination before anesthesia.
Complete sensory examination before anesthesia.
 Note pattern of nail bed laceration (simple/stellate), involvement of germinal matrix, and dorsal roof matrix. (Fig. 3-3 shows a crush injury of the right thumb with a stellate laceration involving the sterile and germinal matrices.)
Note pattern of nail bed laceration (simple/stellate), involvement of germinal matrix, and dorsal roof matrix. (Fig. 3-3 shows a crush injury of the right thumb with a stellate laceration involving the sterile and germinal matrices.)
 Look out for associated subtotal pulp amputation (Fig. 3-4).
Look out for associated subtotal pulp amputation (Fig. 3-4).



Surgical Anatomy
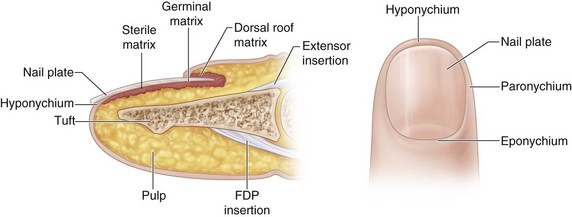
 The nail is a hard structure composed of desiccated, keratinized, squamous cells attached to the nail bed and is the end product of the nail bed’s generative efforts. The nail is loosely attached to the germinal matrix but is densely adherent to the underlying sterile matrix and the eponychium.
The nail is a hard structure composed of desiccated, keratinized, squamous cells attached to the nail bed and is the end product of the nail bed’s generative efforts. The nail is loosely attached to the germinal matrix but is densely adherent to the underlying sterile matrix and the eponychium.
 The nail bed is composed of sterile matrix, germinal matrix, and dorsal roof matrix (Fig. 3-6).
The nail bed is composed of sterile matrix, germinal matrix, and dorsal roof matrix (Fig. 3-6).




Exposures
 A Freer elevator is inserted between the nail plate and the nail bed distally and used to elevate the nail plate off the nail bed from distal to proximal.
A Freer elevator is inserted between the nail plate and the nail bed distally and used to elevate the nail plate off the nail bed from distal to proximal.
 Nail bed lacerations that extend under the nail fold or involve the germinal matrix require elevation of the dorsal roof matrix to expose the laceration and allow a good repair. This is done by making two oblique incisions at the corner of the nail fold and elevating the dorsal roof matrix as a proximally based flap. Two sutures at either corner maintain the flap in position (Fig. 3-7).
Nail bed lacerations that extend under the nail fold or involve the germinal matrix require elevation of the dorsal roof matrix to expose the laceration and allow a good repair. This is done by making two oblique incisions at the corner of the nail fold and elevating the dorsal roof matrix as a proximally based flap. Two sutures at either corner maintain the flap in position (Fig. 3-7).

Pearls
In children, general anesthesia is required to facilitate a meticulous repair.
If the laceration involves only the distal portion of sterile matrix, the nail plate needs to be elevated only 1 to 2 mm beyond the laceration.
Examine the undersurface of the nail for any nail bed remnants. They can be used as a free graft.
When the dorsal roof matrix flap is sutured back, it is important to ensure that the suture passes through the full thickness of the tissue.





