Fig. 1
(a) Immediate posttraumatic X-rays. (b) X-rays after debridement, compression and application of unilateral external fixator. (c) Clinical photo of the leg after healing of the soft tissue. (d) Immediate pre-operative clinical photo
3 Preoperative Problem List
1.
The presence of a huge bone defect
2.
Lost tibial and fibular elements of the ankle joint
4 Treatment Strategy
Five eighth and one Ilizarov ring were mounted to the upper tibia and another ring applied to the middle part using 2 mm K-wires. A foot frame was applied to the calcaneus and forefoot. The leg was kept fixed in the shortened position, which allowed closure of the soft tissue in the first operation. Corticotomy was performed in the upper tibia, and the waiting period was 2 weeks. Then, distraction started at a rate of 1 mm per day and modified according to the regenerate formation till the lower tibial part reached the docking site. There was anterior displacement of the lower tibia, so the frame was modified to allow for sagittal plane correction of the displacement. After that, lengthening was continued from the upper ring till the leg length was equal on both sides.
5 Basic Principles
Acute shortening is a valid option for managing the bone and soft tissue defects . This principle was applied to close the skin and soft tissue defect and to minimize the bone gap. Distraction histogenesis is the mainstay of treatment of bone defects.
6 Images During Treatment
See Fig. 2
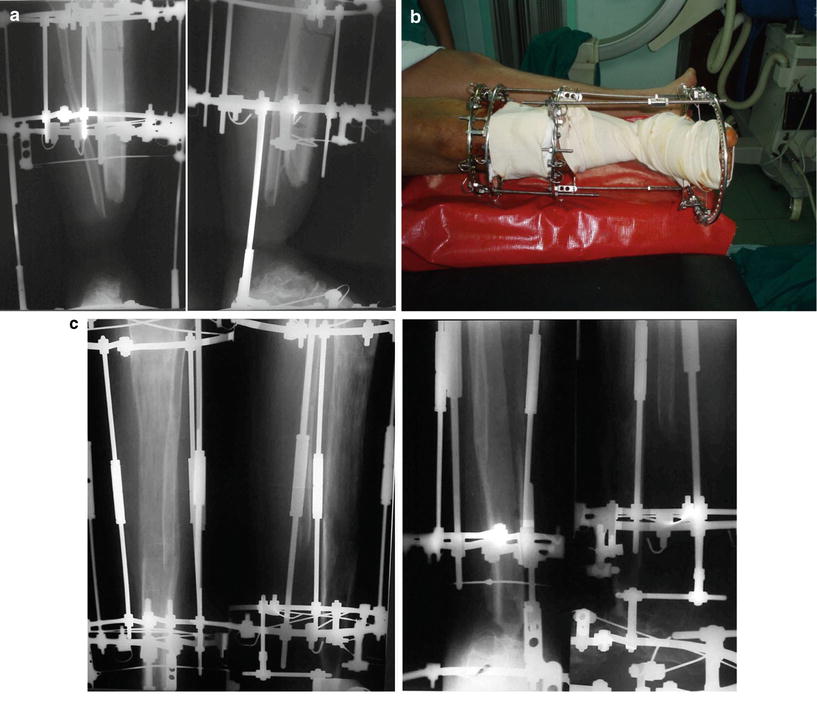
Fig. 2
 6: A 10 cm Traumatic Femoral Defect Treated with a Transport Technique Followed by a Lengthening Procedure. Sequential Use of a Monotube External Fixator and an Intramedullary Rod
6: A 10 cm Traumatic Femoral Defect Treated with a Transport Technique Followed by a Lengthening Procedure. Sequential Use of a Monotube External Fixator and an Intramedullary Rod
 28: Proximal Tibial Bone Defect Treated with Intentional Deformity and Bone Transport
28: Proximal Tibial Bone Defect Treated with Intentional Deformity and Bone Transport
 30: C3.3 Pilon Fracture Closed. Ilizarov Fixation with Limited Open Reduction of Joint Surface and Distal Tibia Bridging Distraction of Ankle Joint
30: C3.3 Pilon Fracture Closed. Ilizarov Fixation with Limited Open Reduction of Joint Surface and Distal Tibia Bridging Distraction of Ankle Joint
 78: Two-Stage Treatment of a Chronic Foot Dislocation
78: Two-Stage Treatment of a Chronic Foot Dislocation
 84: Lapidus Fusion with External Fixation
84: Lapidus Fusion with External Fixation
 65: Closed Correction of Club Foot with Ilizarov
65: Closed Correction of Club Foot with Ilizarov




Related posts:
6: A 10 cm Traumatic Femoral Defect Treated with a Transport Technique Followed by a Lengthening Procedure. Sequential Use of a Monotube External Fixator and an Intramedullary Rod
28: Proximal Tibial Bone Defect Treated with Intentional Deformity and Bone Transport
30: C3.3 Pilon Fracture Closed. Ilizarov Fixation with Limited Open Reduction of Joint Surface and Distal Tibia Bridging Distraction of Ankle Joint
78: Two-Stage Treatment of a Chronic Foot Dislocation
84: Lapidus Fusion with External Fixation
65: Closed Correction of Club Foot with Ilizarov
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
