Fig. 1
Pre-operative anteroposterior (a) and lateral (b) view radiographs (Copyright 2014, Rubin Institute for Advanced Orthopedics, Sinai Hospital of Baltimore)

Fig. 2
Pre-operative anteroposterior (a) and lateral (b) view clinical photographs (Copyright 2014, Rubin Institute for Advanced Orthopedics, Sinai Hospital of Baltimore)
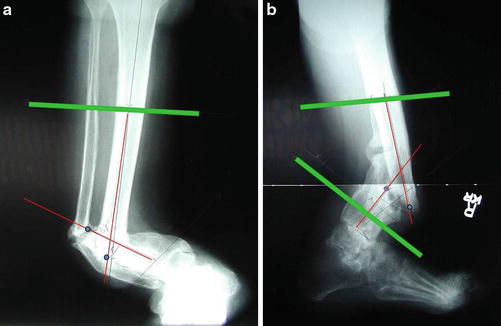
Fig. 3
Pre-operative anteroposterior (a) and lateral (b) view radiographs show deformity parameters (fracture method) (Copyright 2014, Rubin Institute for Advanced Orthopedics, Sinai Hospital of Baltimore)
3 Preoperative Problem List
Severe deformity
Long duration
Rheumatoid arthritis and diabetes mellitus
4 Treatment Strategy
Gradual deformity correction was combined with minimally invasive fixation. The foot was included when planning the deformity correction. Ankle range of motion was preserved, but the foot was included in the frame. The hypertrophic nonunion was distracted 0.5 mm/day at the concavity of the deformity. Additional bone grafting was not needed because the distraction allowed the regenerate process to occur. A cast was applied after frame removal to provide support and remained in place for 1 month.
5 Basic Principles
Gradually correct the deformity to avoid neurovascular injury. Also allow the hypertrophic nonunion to heal without bone graft. Address the ankle to avoid development of any equinus deformity. Include the foot in the frame for stability.
6 Images During Treatment
See Figs. 4
 8: Femoral Bone Defect
8: Femoral Bone Defect
 28: Proximal Tibial Bone Defect Treated with Intentional Deformity and Bone Transport
28: Proximal Tibial Bone Defect Treated with Intentional Deformity and Bone Transport
 30: C3.3 Pilon Fracture Closed. Ilizarov Fixation with Limited Open Reduction of Joint Surface and Distal Tibia Bridging Distraction of Ankle Joint
30: C3.3 Pilon Fracture Closed. Ilizarov Fixation with Limited Open Reduction of Joint Surface and Distal Tibia Bridging Distraction of Ankle Joint
 78: Two-Stage Treatment of a Chronic Foot Dislocation
78: Two-Stage Treatment of a Chronic Foot Dislocation
 84: Lapidus Fusion with External Fixation
84: Lapidus Fusion with External Fixation
 65: Closed Correction of Club Foot with Ilizarov
65: Closed Correction of Club Foot with Ilizarov




Related posts:
8: Femoral Bone Defect
28: Proximal Tibial Bone Defect Treated with Intentional Deformity and Bone Transport
30: C3.3 Pilon Fracture Closed. Ilizarov Fixation with Limited Open Reduction of Joint Surface and Distal Tibia Bridging Distraction of Ankle Joint
78: Two-Stage Treatment of a Chronic Foot Dislocation
84: Lapidus Fusion with External Fixation
65: Closed Correction of Club Foot with Ilizarov
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
