Procedure 2 Fasciotomy of the Upper Limb




Examination/Imaging
Clinical Examination
 Compartment syndrome is caused by increased pressure within the myofascial compartments leading to a decrease in blood flow. Nerves followed by muscle are most sensitive to ischemia and undergo irreversible changes within 6 to 8 hours. It is therefore important to decompress the fascial compartment by performing a fasciotomy and to restore tissue perfusion as soon as possible.
Compartment syndrome is caused by increased pressure within the myofascial compartments leading to a decrease in blood flow. Nerves followed by muscle are most sensitive to ischemia and undergo irreversible changes within 6 to 8 hours. It is therefore important to decompress the fascial compartment by performing a fasciotomy and to restore tissue perfusion as soon as possible.

 A prophylactic fasciotomy should be performed in all major limb replantations/revascularizations irrespective of the clinical appearance of the limb at the end of the procedure (Fig. 2-4). The limb is insensate and becomes progressively swollen as a result of diminished venous return and ischemia reperfusion injury. When a fasciotomy is not performed, the arterial inflow can be compromised, leading to failure of the replantation.
A prophylactic fasciotomy should be performed in all major limb replantations/revascularizations irrespective of the clinical appearance of the limb at the end of the procedure (Fig. 2-4). The limb is insensate and becomes progressively swollen as a result of diminished venous return and ischemia reperfusion injury. When a fasciotomy is not performed, the arterial inflow can be compromised, leading to failure of the replantation.


Investigations
 No investigations are required if a diagnosis of compartment syndrome is clinically apparent. Some laboratory studies (complete blood count, prothrombin time, partial thromboplastin time, serum and urine myoglobin, and creatinine phosphokinase) and imaging studies (radiographs, Doppler, and arteriography) can be used to complement the clinical findings.
No investigations are required if a diagnosis of compartment syndrome is clinically apparent. Some laboratory studies (complete blood count, prothrombin time, partial thromboplastin time, serum and urine myoglobin, and creatinine phosphokinase) and imaging studies (radiographs, Doppler, and arteriography) can be used to complement the clinical findings.
 If a clinical diagnosis is equivocal, compartment pressure measurements should be obtained. We use a commercially available device (Stryker Intra-Compartmental Pressure Monitor) (Fig. 2-5). The normal tissue pressure is 0 to 8 mm Hg. A fasciotomy is recommended if the tissue pressure is higher than 30 mm Hg. Close monitoring, repeated clinical examination, and serial measurement of compartment pressures may be required for pressure measurements between 20 and 30 mm Hg.
If a clinical diagnosis is equivocal, compartment pressure measurements should be obtained. We use a commercially available device (Stryker Intra-Compartmental Pressure Monitor) (Fig. 2-5). The normal tissue pressure is 0 to 8 mm Hg. A fasciotomy is recommended if the tissue pressure is higher than 30 mm Hg. Close monitoring, repeated clinical examination, and serial measurement of compartment pressures may be required for pressure measurements between 20 and 30 mm Hg.

Surgical Anatomy
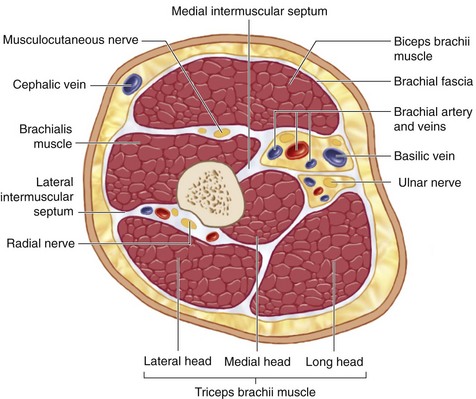
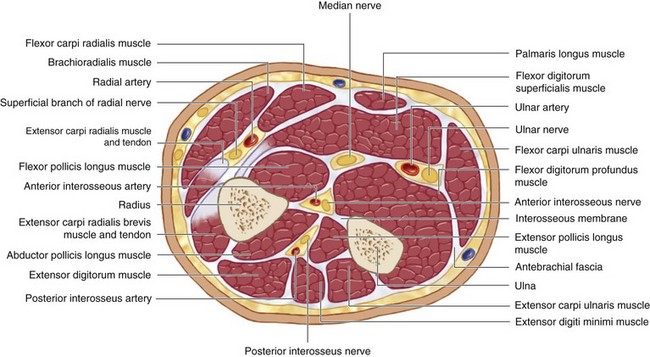
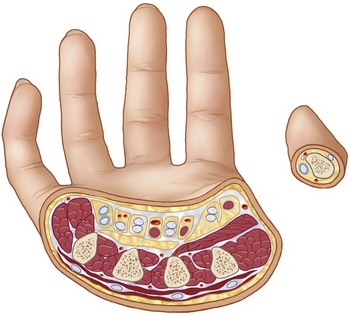
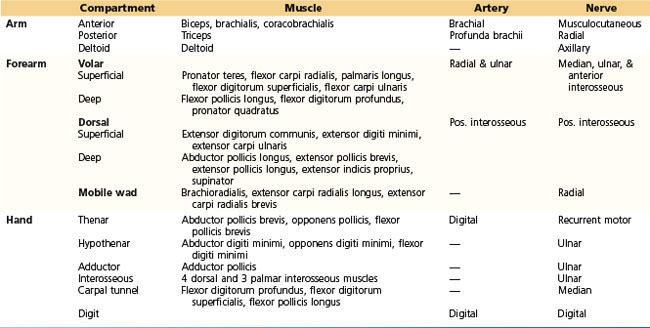
 The myofascial compartments of the upper extremity may be divided into compartments of the arm, forearm, and hand (Figs. 2-6, 2-7, and 2-8). The compartments and their contents are listed in Table 2-1.
The myofascial compartments of the upper extremity may be divided into compartments of the arm, forearm, and hand (Figs. 2-6, 2-7, and 2-8). The compartments and their contents are listed in Table 2-1.

Positioning
 The procedure is performed under tourniquet control and regional or general anesthesia. The patient is positioned supine with the affected extremity on a hand table. A fasciotomy is usually done at the end of major limb replantation, and a tourniquet is not used in this situation. An emergency escharotomy may be done at the bedside for a circumferential third-degree burn because such a burn is not painful.
The procedure is performed under tourniquet control and regional or general anesthesia. The patient is positioned supine with the affected extremity on a hand table. A fasciotomy is usually done at the end of major limb replantation, and a tourniquet is not used in this situation. An emergency escharotomy may be done at the bedside for a circumferential third-degree burn because such a burn is not painful.
Exposures
Hand
 The carpal tunnel is decompressed by a single incision between the thenar and hypothenar muscles in line with the third web space (Fig. 2-9).
The carpal tunnel is decompressed by a single incision between the thenar and hypothenar muscles in line with the third web space (Fig. 2-9).
 The thenar compartment is decompressed by an oblique longitudinal incision along the radial margin of the thenar eminence (see Fig. 2-9).
The thenar compartment is decompressed by an oblique longitudinal incision along the radial margin of the thenar eminence (see Fig. 2-9).
 The hypothenar compartment is released via a longitudinal incision along the ulnar aspect of the palm (see Fig. 2-9).
The hypothenar compartment is released via a longitudinal incision along the ulnar aspect of the palm (see Fig. 2-9).
Related posts:
 28: Pronator Teres Rerouting
28: Pronator Teres Rerouting
 33: Correction of Swan-Neck Deformity in the Rheumatoid Hand
33: Correction of Swan-Neck Deformity in the Rheumatoid Hand
 89: Total Wrist Fusion
89: Total Wrist Fusion
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


