Fig. 1
Standing 51” hip-to-ankle X-ray. Mechanical alignment is within normal limits, Note the patient has a 5 cm block under his right foot in order to level his pelvis
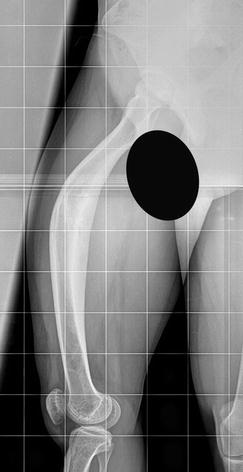
Fig. 2
Lateral X-ray of the right femur demonstrating an apex anterior mid-diaphyseal deformity
3 Preoperative Problem List
1.
Right femur 40° procurvatum deformity
2.
4.5 cm limb length discrepancy
3.
Sciatic nerve at risk
4 Treatment Strategy
1.
Peroneal nerve release (do not close the wound, monitor nerve tension during surgery)
2.
Open wedge resection (location and size previously planned)
3.
Proximal fragment reaming
4.
Distal fragment reaming through osteotomy
5.
Nail insertion
6.
Autograft application (from resected wedge)
5 Basic Principles
The surgical planning should consider a wedge with an angle equal to the angle to correct. Its apex should be located posteriorly in the bone (closed wedge) to keep the bone length. In case a concern of sciatic nerve stretching exists, the apex should be located at the posterior soft tissues (trapezoid bone wedge). In that case, less nerve stretching will take place. Temporary anterior and lateral external fixation (fixator-assisted nailing) is an option during the surgery to help with reduction and maintain rotational alignment (not used in this case). A lengthening will be performed at a second stage as needed to achieve femoral length equality. An alternative would have been to do a percutaneous osteotomy and perform a gradual correction using a Taylor spatial frame. However, following patient desires to avoid external fixation, a staged procedure was elected as the treatment method.
6 Images During Treatment
See Figs. 3, 4, 5, 6, 7, and 8
 8: Femoral Bone Defect
8: Femoral Bone Defect
 11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
 30: C3.3 Pilon Fracture Closed. Ilizarov Fixation with Limited Open Reduction of Joint Surface and Distal Tibia Bridging Distraction of Ankle Joint
30: C3.3 Pilon Fracture Closed. Ilizarov Fixation with Limited Open Reduction of Joint Surface and Distal Tibia Bridging Distraction of Ankle Joint
 78: Two-Stage Treatment of a Chronic Foot Dislocation
78: Two-Stage Treatment of a Chronic Foot Dislocation
 84: Lapidus Fusion with External Fixation
84: Lapidus Fusion with External Fixation
 65: Closed Correction of Club Foot with Ilizarov
65: Closed Correction of Club Foot with Ilizarov




Related posts:
8: Femoral Bone Defect
11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
30: C3.3 Pilon Fracture Closed. Ilizarov Fixation with Limited Open Reduction of Joint Surface and Distal Tibia Bridging Distraction of Ankle Joint
78: Two-Stage Treatment of a Chronic Foot Dislocation
84: Lapidus Fusion with External Fixation
65: Closed Correction of Club Foot with Ilizarov
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
