Fig. 1
Clinical photograph of the patient standing showing large varus deformity. The patient maintained his left knee flexed in order to accommodate for the short right lower extremity. Note the valgus-compensated right ankle and subtalar joint to maintain a plantigrade foot. The pre-operative clinical exam demonstrated a flexible foot deformity, which indicated that the hindfoot valgus would resolve as the tibia vara was corrected
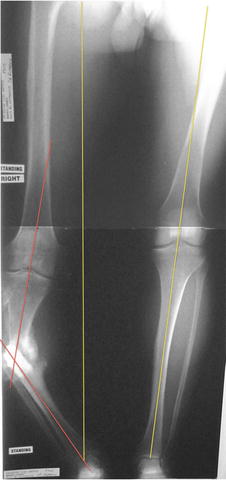
Fig. 2
Pre-operative standing 51″ erect leg radiograph. Mechanical axis deviation (MAD) on the right was 78 mm medial to midline; left was 0 mm (yellow lines). The center of rotation of angulation (CORA) was at the obvious tibial nonunion site (red lines), and its magnitude was 40° of varus

Fig. 3
Pre-operative (a) AP and (b) lateral tibial X-rays. Magnitudes of deformity were 40° of varus, 11° of procurvatum, and 14 mm of anterior translation. The apex of deformity was distal to the nonunion on the lateral X-ray since there was an associated anterior translation deformity
3 Preoperative Problem List
1.
Hypertrophic “stiff” tibial nonunion , right
2.
History of infection, right tibia
3.
40° tibia vara
4.
11° tibial procurvatum deformity
5.
14 mm anterior tibial translation deformity
6.
3.2 cm LLD , right short
7.
Cigarette smoking
8.
Alcohol abuse
4 Treatment Strategy
The surgical strategy was based on the clinical assumption that the nonunion occurred because of persistent instability and sheer forces, despite a favorable biological milieu – that is, a hypertrophic or stiff nonunion. Under anesthesia, after fibular osteotomy, the patient’s tibia was examined to confirm the pre-operative hypothesis. The nonunion was tested and there was less than 5° of motion. This confirmed that it was a stiff nonunion, and we thus proceeded with the closed nonunion repair . This consisted of gradual distraction through the nonunion site, stimulating the nonunion, and gradual correction of varus, procurvatum, and anterior translation. Residual LLD would be analyzed after complete deformity correction as length will be achieved by resolving varus and procurvatum. Once the distraction phase was complete, the nonunion site was compressed to augment bone healing while in the consolidation phase.
5 Basic Principles
Related posts:
 8: Femoral Bone Defect
8: Femoral Bone Defect
 11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
 30: C3.3 Pilon Fracture Closed. Ilizarov Fixation with Limited Open Reduction of Joint Surface and Distal Tibia Bridging Distraction of Ankle Joint
30: C3.3 Pilon Fracture Closed. Ilizarov Fixation with Limited Open Reduction of Joint Surface and Distal Tibia Bridging Distraction of Ankle Joint
 78: Two-Stage Treatment of a Chronic Foot Dislocation
78: Two-Stage Treatment of a Chronic Foot Dislocation
 84: Lapidus Fusion with External Fixation
84: Lapidus Fusion with External Fixation
 65: Closed Correction of Club Foot with Ilizarov
65: Closed Correction of Club Foot with Ilizarov
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


