Figure 13.1
Impetigo, a “honey crusted” covering an erythematous base
Clinical Differential Diagnosis
Impetigo
Contact dermatitis
Scabies
Candidiasis
Diagnosis
IMPETIGO (bacterial) is a common infection of the skin that is highly contagious. It is divided into two categories: nonbullous and bullous impetigo. Nonbullous impetigo is the more common form that is responsible for 70 % of cases and occurs in individuals of all ages. It is usually caused by Staphylococcus aureus or Group A beta-hemolytic streptococcus (Streptococcus pyogenes). The lesions begin as vesicles that quickly rupture and produce a characteristic honey-colored crust.
Bullous impetigo is caused by Staphylococcus aureus and is more likely to affect neonates and older infants. These lesions also begin as vesicles that quickly enlarge to form bullae containing clear or yellowish fluid. After 2 or 3 days these bullae rupture and form light brown crusts that border erythematous erosions. The lesions are usually painless and heal without scarring. Some patients complain of pruritus or a burning sensation. Microscopically, the vesicle is separated at the level of the stratum corneum which contains a few trapped neutrophils (Fig. 13.2).
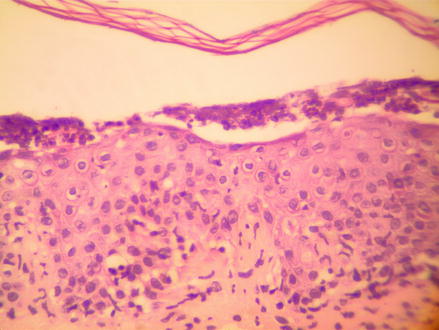
Figure 13.2
H&E 100×. Bacteria infection, Impetigo
Impetigo usually occurs around the nose and the mouth and is also frequently seen on exposed extremities. It develops at sites of minor skin trauma like abrasions that permit “impetiginzation” or introduction of the infection. Impetigo tends to affect individuals with compromised skin barriers and immune systems like those with atopic dermatitis and diabetes. Streptococcal impetigo is seen more often in warm, humid climates, during the summer months, and spreads quickly in overcrowded environments.
In bullous impetigo, S aureus produces an exfoliative toxin that causes the development of the bulla. Methicillin-resistant S aureus is becoming an increasingly common etiologic agent. In industrialized countries, mixed infections are becoming more frequent, as well. Typically the infection begins as a streptococcal infection that is then secondarily infected by S aureus.
Related posts:
 6 Year Old White Male with Recurrent Brownish Patches Around Mouth
6 Year Old White Male with Recurrent Brownish Patches Around Mouth
 70 Year Old White Male with Grouped Blisters on Right Lower Leg
70 Year Old White Male with Grouped Blisters on Right Lower Leg
 50 Year Old Male with Confluent, Scaly Plaque Covering the Inguinal Area and Extending to Both Inner Thighs
50 Year Old Male with Confluent, Scaly Plaque Covering the Inguinal Area and Extending to Both Inner Thighs
 6 Year Old White Boy with a Rash on Buttock
6 Year Old White Boy with a Rash on Buttock
 57 Year Old Male with Multiple Widespread Excoriations
57 Year Old Male with Multiple Widespread Excoriations
 46 Year Old Female with Multiple Slightly Eroded Reddish Papules on Her Arm
46 Year Old Female with Multiple Slightly Eroded Reddish Papules on Her Arm
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


