Procedure 18 Tendon Transfers for Carpal Tunnel Syndrome
 See Video 14: Tendon Transfer for Anterior Interosseous Nerve Palsy (FDS to FPL)
See Video 14: Tendon Transfer for Anterior Interosseous Nerve Palsy (FDS to FPL)





Examination/Imaging
Clinical Examination
 Sensation: It is important to document the level of sensation in the thumb and fingers preoperatively. Patients may also have diminished sensation in the ulnar nerve distribution. The potential functional benefit of a tendon transfer will be diminished in a patient with sensory loss, and these patients must be counseled about the likely poorer outcome after surgery.
Sensation: It is important to document the level of sensation in the thumb and fingers preoperatively. Patients may also have diminished sensation in the ulnar nerve distribution. The potential functional benefit of a tendon transfer will be diminished in a patient with sensory loss, and these patients must be counseled about the likely poorer outcome after surgery.



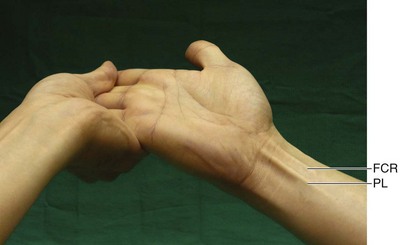
 We use the test described by Mishra to determine the presence of the PL. The traditional test described by Schaeffer requires the patient to abduct and oppose the thumb to the small finger and flex the wrist. A patient with thenar atrophy will find it difficult to do so. The Mishra test is performed by holding the patient’s wrist and fingers in hyperextension, while asking the patient to flex the wrist. This stretches the palmar aponeurosis and makes the PL taut when the patient attempts wrist flexion (Fig. 18-1).
We use the test described by Mishra to determine the presence of the PL. The traditional test described by Schaeffer requires the patient to abduct and oppose the thumb to the small finger and flex the wrist. A patient with thenar atrophy will find it difficult to do so. The Mishra test is performed by holding the patient’s wrist and fingers in hyperextension, while asking the patient to flex the wrist. This stretches the palmar aponeurosis and makes the PL taut when the patient attempts wrist flexion (Fig. 18-1).


Surgical Anatomy
 Thumb opposition is a complex movement produced by a combination of flexion, palmar abduction, and pronation and requires participation of both the MCP and CMC joints. The prime muscle of thumb opposition is believed to be the APB with contributions from the OP and flexor pollicis brevis (FPB).
Thumb opposition is a complex movement produced by a combination of flexion, palmar abduction, and pronation and requires participation of both the MCP and CMC joints. The prime muscle of thumb opposition is believed to be the APB with contributions from the OP and flexor pollicis brevis (FPB).

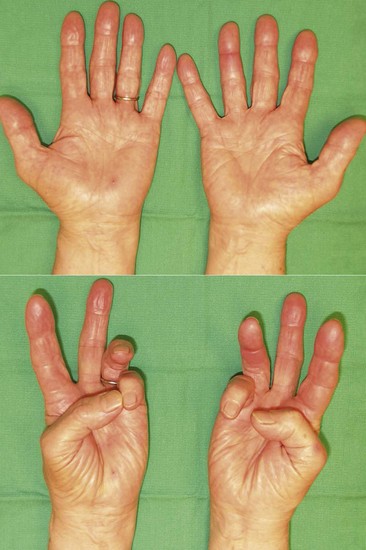
 Reasonable thumb abduction and opposition may be retained after isolated median nerve injury or severe carpal tunnel syndrome as a result of preserved ulnar nerve function (retained innervation of the deep head of the FPB and variability in thenar muscle innervation by connection between the ulnar and median nerves). Figure 18-2 shows the preoperative appearance of the hand with severe CST on the right. Note the thenar atrophy and inability to palmarly abduct the right thumb.
Reasonable thumb abduction and opposition may be retained after isolated median nerve injury or severe carpal tunnel syndrome as a result of preserved ulnar nerve function (retained innervation of the deep head of the FPB and variability in thenar muscle innervation by connection between the ulnar and median nerves). Figure 18-2 shows the preoperative appearance of the hand with severe CST on the right. Note the thenar atrophy and inability to palmarly abduct the right thumb.

Positioning
 The procedure is performed under tourniquet control. It is usually performed under sedation and local anesthesia because this procedure is rather expedient and there is no need to take unnecessary anesthetic risk in elderly patients. The patient is positioned supine with the affected extremity on a hand table.
The procedure is performed under tourniquet control. It is usually performed under sedation and local anesthesia because this procedure is rather expedient and there is no need to take unnecessary anesthetic risk in elderly patients. The patient is positioned supine with the affected extremity on a hand table.





