Procedure 17 Surgical Treatment of Neuromas in the Hand
Indications
 Neuroma with the following characteristics:
Neuroma with the following characteristics:
 A neuroma can result from the following:
A neuroma can result from the following:
Examination/Imaging
Clinical Examination
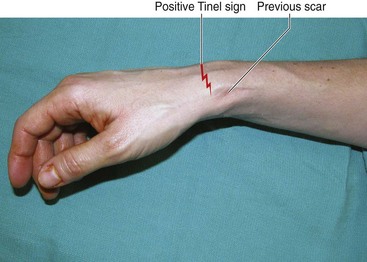
 Patients may present with pain associated with scar and altered sensation (hypoesthesia, hyperalgesia, or anesthesia). The pain may be spontaneous or result from pressure over the neuroma, movement of adjacent joints, or light touch in the vicinity of the neuroma.
Patients may present with pain associated with scar and altered sensation (hypoesthesia, hyperalgesia, or anesthesia). The pain may be spontaneous or result from pressure over the neuroma, movement of adjacent joints, or light touch in the vicinity of the neuroma.

 The location of the neuroma in relation to any overlying scar and the presence of a Tinel sign must be noted (Fig. 17-1).
The location of the neuroma in relation to any overlying scar and the presence of a Tinel sign must be noted (Fig. 17-1).

Surgical Anatomy
 A neuroma of the hand can be an end neuroma or an in-continuity neuroma. End neuromas are frequently associated with digital amputation and involve the proper digital nerves. In-continuity neuromas most often result from poor surgical repair and involve the median and ulnar nerves at the wrist. Both end neuromas and in-continuity neuromas can also result from unrecognized iatrogenic injury (e.g., superficial radial nerve, palmar cutaneous branch of median nerve) or delayed presentation of a partially or completely divided nerve.
A neuroma of the hand can be an end neuroma or an in-continuity neuroma. End neuromas are frequently associated with digital amputation and involve the proper digital nerves. In-continuity neuromas most often result from poor surgical repair and involve the median and ulnar nerves at the wrist. Both end neuromas and in-continuity neuromas can also result from unrecognized iatrogenic injury (e.g., superficial radial nerve, palmar cutaneous branch of median nerve) or delayed presentation of a partially or completely divided nerve.
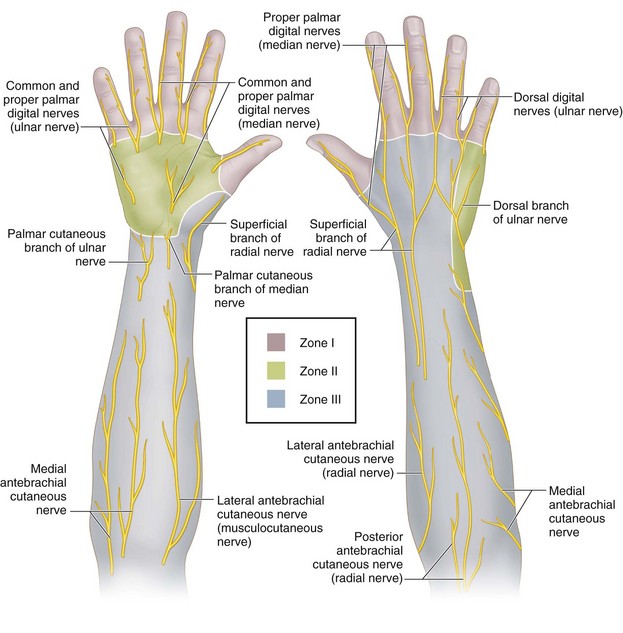
 The hand and wrist have been classified into three zones based on the location of the neuroma (Fig. 17-2). Zone I represents the digits and includes neuromas arising from the digital nerves, their dorsal branches, and the terminal branches of the nerves innervating the dorsum of the hand. Zone II represents the body of the hand and includes the common digital nerves, the palmar cutaneous branches of the median nerve, and the palmar and dorsal cutaneous branches of the ulnar nerve. Zone III represents the radial border of the wrist and forearm and includes the superficial radial nerve, the lateral antebrachial cutaneous nerve, the medial antebrachial cutaneous nerve, and the posterior cutaneous nerve of the forearm.
The hand and wrist have been classified into three zones based on the location of the neuroma (Fig. 17-2). Zone I represents the digits and includes neuromas arising from the digital nerves, their dorsal branches, and the terminal branches of the nerves innervating the dorsum of the hand. Zone II represents the body of the hand and includes the common digital nerves, the palmar cutaneous branches of the median nerve, and the palmar and dorsal cutaneous branches of the ulnar nerve. Zone III represents the radial border of the wrist and forearm and includes the superficial radial nerve, the lateral antebrachial cutaneous nerve, the medial antebrachial cutaneous nerve, and the posterior cutaneous nerve of the forearm.
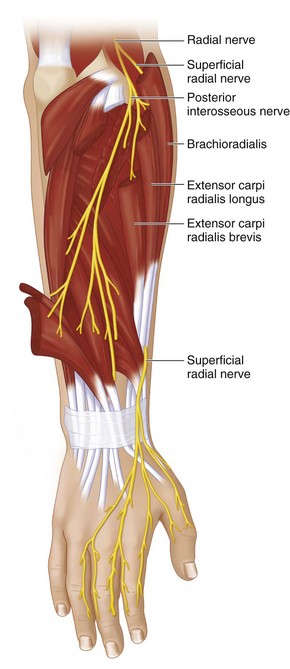
 Although a neuroma can involve any sensory nerve in the hand, the superficial radial nerve is particularly prone to developing a neuroma, and these neuromas are difficult to manage. The nerve becomes subcutaneous about 7 cm proximal to the radial styloid by piercing the fascia between the brachioradialis (BR) and the extensor carpi radialis longus (ECRL) (Fig. 17-3). It is believed that the nerve may be compressed between the tendons of the ECRL and BR. In 3% to 10% of the population, it passes through the tendon of the brachioradialis, tethering it proximally. These factors, combined with its superficial location, may explain the predisposition to iatrogenic injury and neuroma formation.
Although a neuroma can involve any sensory nerve in the hand, the superficial radial nerve is particularly prone to developing a neuroma, and these neuromas are difficult to manage. The nerve becomes subcutaneous about 7 cm proximal to the radial styloid by piercing the fascia between the brachioradialis (BR) and the extensor carpi radialis longus (ECRL) (Fig. 17-3). It is believed that the nerve may be compressed between the tendons of the ECRL and BR. In 3% to 10% of the population, it passes through the tendon of the brachioradialis, tethering it proximally. These factors, combined with its superficial location, may explain the predisposition to iatrogenic injury and neuroma formation.
Treatment Options
• Our surgical treatment of neuromas is based on the availability of an appropriate distal nerve, the local tissue environment, and the anatomic zone of the neuroma.
• If an appropriate distal target is available, we use a nerve graft to bridge the defect caused by resection of the neuroma. If the local tissue environment is not suitable for a nerve graft, we wrap the nerve graft in a vein, an artificial nerve conduit, or a locally transposed fat flap.
• If an appropriate target is not available, we resect the neuroma and relocate the proximal end. The relocation of the proximal end depends on the anatomic zone.
• We have occasionally used the technique of centro-centralization for a digital nerve neuroma. This involves resection of the neuroma and suturing of the digital nerves to each other. Gorkisch and colleagues (1984) suggested dividing one of the digital nerves 5 to 10 mm proximal to the repair site and performing an additional repair. This creates a nerve graft segment and prevents the development of a neuroma at the original nerve repair site (Fig. 17-4).
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


