Procedure 16 Treatment of a Nerve Gap in the Hand
Indications
 A segmental defect in a nerve can result from the following:
A segmental defect in a nerve can result from the following:
 Nerve grafting should be considered in the following cases:
Nerve grafting should be considered in the following cases:

Examination/Imaging
Clinical Examination
 The possibility of nerve grafting should be discussed for all patients in whom a digital nerve injury is suspected. Potential nerve graft sources and their morbidity should also be discussed (detailed later). It is better to avoid harvesting a nerve graft from the same limb in patients who have preexisting nerve-related pain/paresthesia because it adds another nociceptive focus.
The possibility of nerve grafting should be discussed for all patients in whom a digital nerve injury is suspected. Potential nerve graft sources and their morbidity should also be discussed (detailed later). It is better to avoid harvesting a nerve graft from the same limb in patients who have preexisting nerve-related pain/paresthesia because it adds another nociceptive focus.


Surgical Anatomy
 A variety of substitutes have been described for reconstituting nerve defects. They include nerve (autograft/allograft), biological conduits (e.g., vein, muscle), and artificial conduits (e.g., polyglycolic acid, nanofiber).
A variety of substitutes have been described for reconstituting nerve defects. They include nerve (autograft/allograft), biological conduits (e.g., vein, muscle), and artificial conduits (e.g., polyglycolic acid, nanofiber).
 The available nerve autografts include the posterior interosseous nerve (PIN), superficial radial nerve, medial and lateral antebrachial cutaneous nerves, and sural nerve (Fig. 16-4). We do not use the superficial radial nerve or the lateral antebrachial cutaneous nerves because they provide innervation to potentially valuable areas of skin.
The available nerve autografts include the posterior interosseous nerve (PIN), superficial radial nerve, medial and lateral antebrachial cutaneous nerves, and sural nerve (Fig. 16-4). We do not use the superficial radial nerve or the lateral antebrachial cutaneous nerves because they provide innervation to potentially valuable areas of skin.

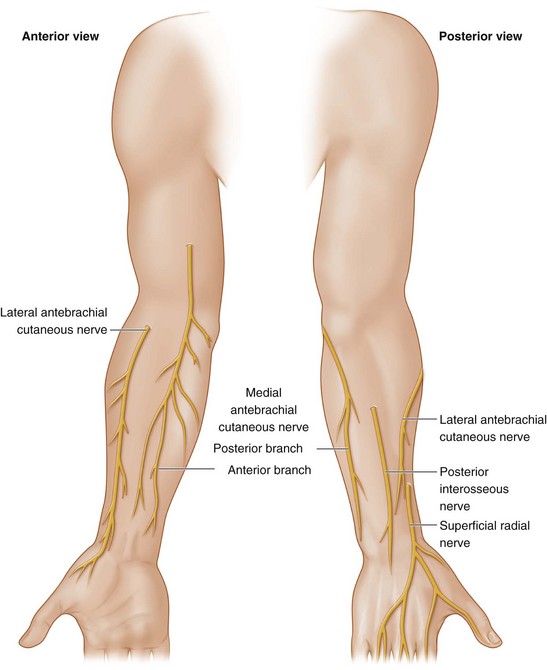
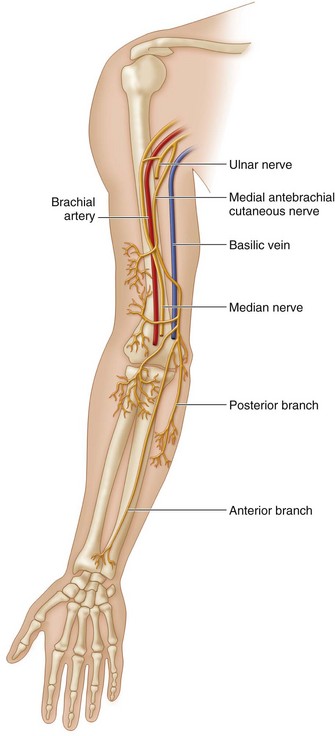
 Medial antebrachial cutaneous nerve (MABCN): This is a purely sensory nerve that arises directly from the medial cord of the brachial plexus (C8, T1) and runs along the axillary vein. It then accompanies the basilic vein in the proximal half of the arm and pierces the deep fascia in the midarm. It splits into anterior and posterior branches in the distal third of the arm. The anterior branch innervates the anteromedial surface of the forearm, whereas the posterior branch innervates the posterior and ulnar aspect of the elbow and forearm (Fig. 16-5). The anterior branch of MABCN is used for nerve graft harvest to avoid sensory loss over the elbow. The anterior branch crosses the elbow between the medial epicondyle and the biceps tendon, usually in front of the antecubital vein, and courses superficial to the flexor carpi ulnaris muscle, ending 10 cm from the wrist. A 20-cm long graft can be harvested based on the anterior branch. It has a cross-sectional area of approximately 0.6 to 1 mm2 and contains three to four fascicles.
Medial antebrachial cutaneous nerve (MABCN): This is a purely sensory nerve that arises directly from the medial cord of the brachial plexus (C8, T1) and runs along the axillary vein. It then accompanies the basilic vein in the proximal half of the arm and pierces the deep fascia in the midarm. It splits into anterior and posterior branches in the distal third of the arm. The anterior branch innervates the anteromedial surface of the forearm, whereas the posterior branch innervates the posterior and ulnar aspect of the elbow and forearm (Fig. 16-5). The anterior branch of MABCN is used for nerve graft harvest to avoid sensory loss over the elbow. The anterior branch crosses the elbow between the medial epicondyle and the biceps tendon, usually in front of the antecubital vein, and courses superficial to the flexor carpi ulnaris muscle, ending 10 cm from the wrist. A 20-cm long graft can be harvested based on the anterior branch. It has a cross-sectional area of approximately 0.6 to 1 mm2 and contains three to four fascicles.
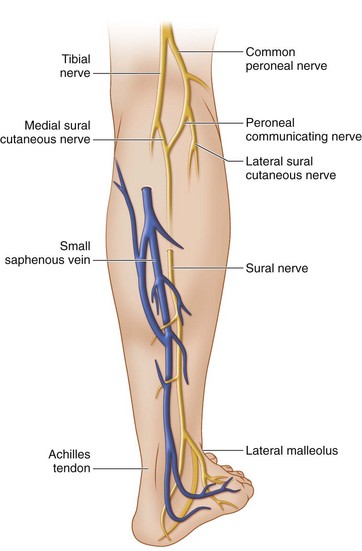
 Sural nerve: The sural nerve is a purely sensory nerve formed by the union of the medial and lateral sural cutaneous nerves (sural communicating nerve). The medial sural cutaneous nerve arises from the tibial nerve and pierces the deep fascia of the leg between the heads of the gastrocnemius in the upper third of the leg. It is then joined by the lateral sural cutaneous nerve branch of the peroneal nerve to form the sural nerve. The sural nerve descends along the lateral margin of the Achilles tendon with the small saphenous vein between the lateral malleolus and the calcaneus (Fig. 16-6). It innervates the lateral aspect of the lower third of the leg and the lateral aspect of the ankle, heel, and foot. A 40-cm–long graft can be harvested based on the sural nerve and medial sural cutaneous nerves. The sural nerve has a cross-sectional area of approximately 2.5 to 3.0 mm2 and contains six to eight fascicles.
Sural nerve: The sural nerve is a purely sensory nerve formed by the union of the medial and lateral sural cutaneous nerves (sural communicating nerve). The medial sural cutaneous nerve arises from the tibial nerve and pierces the deep fascia of the leg between the heads of the gastrocnemius in the upper third of the leg. It is then joined by the lateral sural cutaneous nerve branch of the peroneal nerve to form the sural nerve. The sural nerve descends along the lateral margin of the Achilles tendon with the small saphenous vein between the lateral malleolus and the calcaneus (Fig. 16-6). It innervates the lateral aspect of the lower third of the leg and the lateral aspect of the ankle, heel, and foot. A 40-cm–long graft can be harvested based on the sural nerve and medial sural cutaneous nerves. The sural nerve has a cross-sectional area of approximately 2.5 to 3.0 mm2 and contains six to eight fascicles.
Positioning
 The procedure is performed under tourniquet control using 3.0× to 3.5× loupe magnification for the initial dissection and an operating microscope for the nerve repairs.
The procedure is performed under tourniquet control using 3.0× to 3.5× loupe magnification for the initial dissection and an operating microscope for the nerve repairs.
 The patient is positioned supine with the affected extremity on a hand table.
The patient is positioned supine with the affected extremity on a hand table.
 The leg must be prepared and a thigh tourniquet applied, if a sural nerve graft is anticipated.
The leg must be prepared and a thigh tourniquet applied, if a sural nerve graft is anticipated.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


