Fig. 1
Pre-operative X-ray AP view, open comminuted right midshaft tibia and fibula fracture (Gustilo Type IIIC). In addition, there is a fracture of the lateral tibial plateau
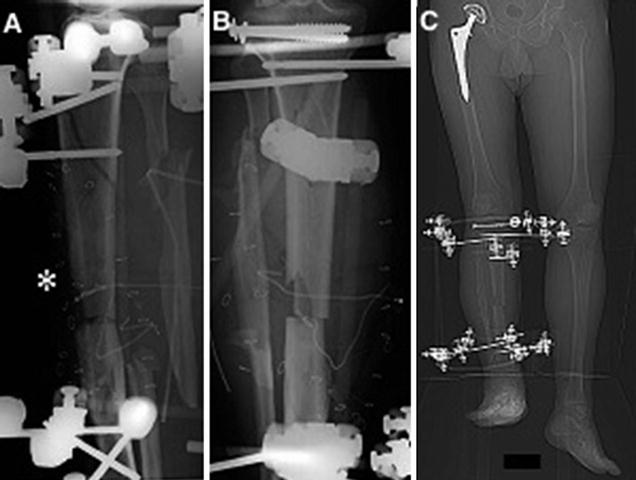
Fig. 2
Post-operative X-ray after primary treatment in AP (a) and lateral (b) view of the right lower limb, (c) CT scanogram with limb shortening of 4.7 cm (1.85 in.)
3 Preoperative Problem List
1.
Nonunion of the open lower leg fracture (Gustilo Type IIIC) 5 months after injury
2.
4.7 cm (1.85 in.) shortening of the right lower limb (1 in. shortening due to right THA after acetabular fracture)
4 Treatment Strategy
(a)
Limb salvage consisted of soft tissue debridement and tibial shortening at the fracture site. The tibial shaft was stabilized initially with a monolateral external fixator, and screw fixation was performed for the tibial condylar fracture. Additionally temporary skin graft was added to cover the soft tissue defect.
(b)
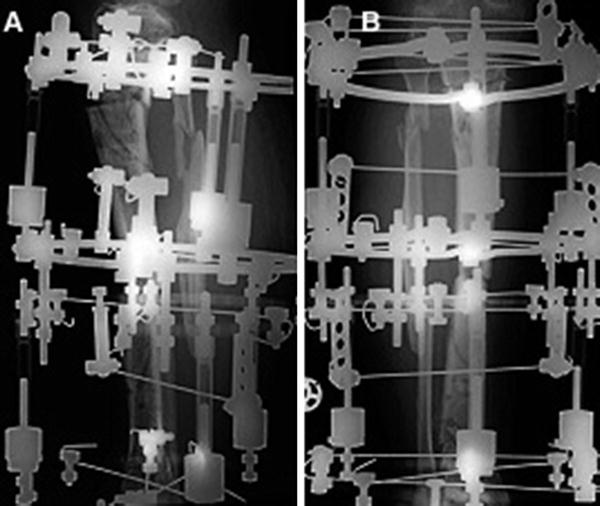
Indication for bifocal callus distraction of the right tibia using a circular frame was established to achieve lower limb equality. Therefore the tibia was osteotomized distally and proximally, with simultaneous compression at the tibial nonunion site. One week after surgery, distraction was started – partial weight bearing was allowed.
5 Basic Principles
1.
The use of acute limb shortening during damage control consists of closing the (bony) defect by compressing the fracture fragments. The safe amount of acute shortening before neurovascular compromise is approximately 3–5 cm in the femur and 2–3 cm in the tibia. Shortening can be greater if this is performed gradually at a rate of 2–3 mm per day. The advantages are that local viable bone is transported acutely into the large bone defect, acute realignment of the fracture is achieved with simultaneous compression of the bone fragments, and viable soft tissue is moved into the zone of injury. There is less need for local and free flaps, and this reduces donor-site morbidity and decreases surgical time because the bone and soft tissue losses are handled at the same time. Furthermore the numbers of docking site revision surgeries may be diminished, limiting adverse event rates.
2.
Distraction osteogenesis involves three different procedures: bone transport, shortening distraction, or both. This may be combined with the use of an intramedullary nail. Therefore, the Ilizarov technique has become the gold standard for the treatment of larger segmental tibial bone defects that require bone lengthening. Depending on the kind and size of bone defects, bone segment transport is the therapy of choice for larger defects, while distraction after optional compression is used for smaller ones.
6 Images During Treatment
See Figs. 3, 4, 5, 6, 7, 8, and 9.
Get Clinical Tree app for offline access
Fig. 3
X-ray lateral (a
 8: Femoral Bone Defect
8: Femoral Bone Defect
 11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
 30: C3.3 Pilon Fracture Closed. Ilizarov Fixation with Limited Open Reduction of Joint Surface and Distal Tibia Bridging Distraction of Ankle Joint
30: C3.3 Pilon Fracture Closed. Ilizarov Fixation with Limited Open Reduction of Joint Surface and Distal Tibia Bridging Distraction of Ankle Joint
 78: Two-Stage Treatment of a Chronic Foot Dislocation
78: Two-Stage Treatment of a Chronic Foot Dislocation
 84: Lapidus Fusion with External Fixation
84: Lapidus Fusion with External Fixation
 65: Closed Correction of Club Foot with Ilizarov
65: Closed Correction of Club Foot with Ilizarov




Related posts:
8: Femoral Bone Defect
11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
30: C3.3 Pilon Fracture Closed. Ilizarov Fixation with Limited Open Reduction of Joint Surface and Distal Tibia Bridging Distraction of Ankle Joint
78: Two-Stage Treatment of a Chronic Foot Dislocation
84: Lapidus Fusion with External Fixation
65: Closed Correction of Club Foot with Ilizarov
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
