Procedure 15 Nerve Transfer Techniques for Elbow Flexion in Brachial Plexus Palsy
 See Video 13: Nerve Transfers for Elbow Flexion in Brachial Plexus Palsy (Ulnar Fascicle to Musculocutaneous Nerve)
See Video 13: Nerve Transfers for Elbow Flexion in Brachial Plexus Palsy (Ulnar Fascicle to Musculocutaneous Nerve)Indications




Examination/Imaging
Clinical Examination
 Examine the involvement of all muscles that contribute to elbow flexion—biceps, brachialis, and brachioradialis—to determine the site of injury (e.g., nerve root versus peripheral nerve).
Examine the involvement of all muscles that contribute to elbow flexion—biceps, brachialis, and brachioradialis—to determine the site of injury (e.g., nerve root versus peripheral nerve).
 Examine the active and passive range of motion at the elbow.
Examine the active and passive range of motion at the elbow.
 Examine the integrity of the vascular supply to the arm.
Examine the integrity of the vascular supply to the arm.
 Examine the integrity of the donor nerve/muscle (e.g., flexor carpi ulnaris).
Examine the integrity of the donor nerve/muscle (e.g., flexor carpi ulnaris).


Positioning
 Position the patient supine with the arm extended onto a surgical arm board.
Position the patient supine with the arm extended onto a surgical arm board.
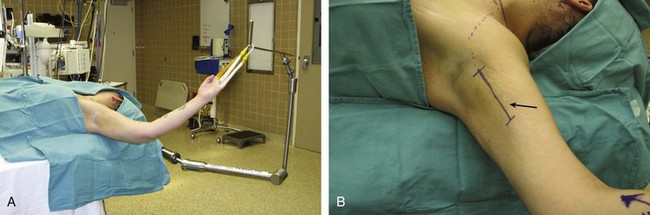
 In patients with decreased shoulder range of motion, an external positioning device can be used to place the arm in abduction and external rotation to reveal the medial aspect of the upper arm (Fig. 15-1).
In patients with decreased shoulder range of motion, an external positioning device can be used to place the arm in abduction and external rotation to reveal the medial aspect of the upper arm (Fig. 15-1).
Exposures
 Ulnar fascicle to musculocutaneous nerve: An incision is made along the medial arm from the pectoralis muscle insertion site to distally, with the incision overlying the path of the neurovascular bundle that lies between the biceps and triceps (see Fig. 15-1).
Ulnar fascicle to musculocutaneous nerve: An incision is made along the medial arm from the pectoralis muscle insertion site to distally, with the incision overlying the path of the neurovascular bundle that lies between the biceps and triceps (see Fig. 15-1).
 Double fascicular nerve transfer for elbow flexion:
Double fascicular nerve transfer for elbow flexion:
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


