Fig. 1
(a) Pre-operative clinical photos of the patient from the side and (b) closeup image. Patient was transferred to our care in a damage control trauma “external fixator” providing traveling traction. Skin invagination (red arrow) is evident in the bone defect site
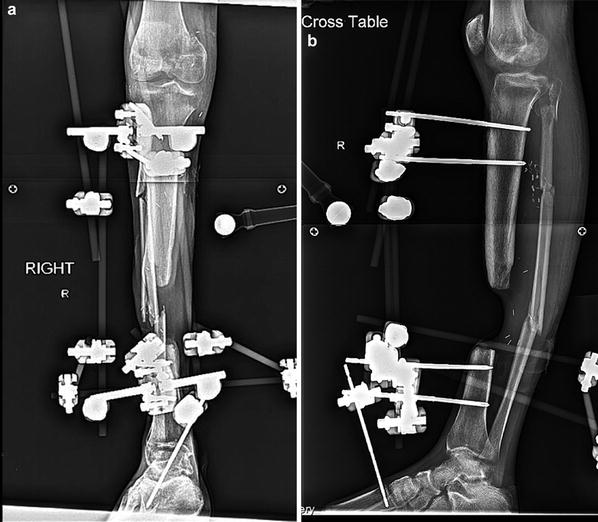
Fig. 2
(a) AP and (b) lateral X-rays of the patient’s right tibia. 6.8 cm total bone loss of the right lower extremity was evident. Axial, coronal, and sagittal alignment were well maintained during the initial limb salvage treatment
3 Preoperative Problem List
1.
Soft tissue invagination status post free flap in distal right leg
2.
Bone defect, right tibia, mid-distal third of the leg, 6.8 cm
3.
Knee contracture
4.
Ankle contracture
5.
Foot drop
6.
Toe contractures
7.
Status post, spanning knee and ankle frame right lower extremity
4 Treatment Strategy
Our limb reconstruction treatment strategy was aimed at treating the bone defect with a bifocal bone transport using a 2-level stacked Taylor Spatial Frame . The soft tissue invagination into the defect was to be managed without a formal elevation. Instead we anticipated that the transporting bone segment into the defect would expand the soft tissue, and the pliability and slow transport rate would accommodate elevation without skin breakdown. This requires bimonthly monitoring in the clinic during treatment. The plan entailed a formal elevation of the soft tissue flap and bone grafting of the docking site with the help of a plastic and reconstruction surgeon. A manipulation under anesthesia of the knee and ankle and flexor tenotomies of the toes were performed at the index surgery. The ankle joint was not spanned; ambulation during treatment was encouraged.
5 Basic Principles
1.
Place proximal and distal rings perpendicular to their respective mechanical axes.
2.
Measure and plan the distance between most distal ring block and transport ring segment. When using the TSF, there is a minimal distal that the smallest struts can shorten. The XXS (extra extra short) TSF struts collapse to 59 mm. Alternatively, Ilizarov rods can be mounted if additional compression is needed and the TSF strut cannot collapse further.
3.
Carefully monitor the soft tissue during transport; a plastic surgeon should be involved early in treatment in the event earlier elevation of the flap is necessary.
4.
Residual deformity during transport can be corrected with a new TSF program. Typical deformities that develop are procurvatum and valgus.
5.
 8: Femoral Bone Defect
8: Femoral Bone Defect
 28: Proximal Tibial Bone Defect Treated with Intentional Deformity and Bone Transport
28: Proximal Tibial Bone Defect Treated with Intentional Deformity and Bone Transport
 30: C3.3 Pilon Fracture Closed. Ilizarov Fixation with Limited Open Reduction of Joint Surface and Distal Tibia Bridging Distraction of Ankle Joint
30: C3.3 Pilon Fracture Closed. Ilizarov Fixation with Limited Open Reduction of Joint Surface and Distal Tibia Bridging Distraction of Ankle Joint
 78: Two-Stage Treatment of a Chronic Foot Dislocation
78: Two-Stage Treatment of a Chronic Foot Dislocation
 84: Lapidus Fusion with External Fixation
84: Lapidus Fusion with External Fixation
 65: Closed Correction of Club Foot with Ilizarov
65: Closed Correction of Club Foot with Ilizarov




Related posts:
8: Femoral Bone Defect
28: Proximal Tibial Bone Defect Treated with Intentional Deformity and Bone Transport
30: C3.3 Pilon Fracture Closed. Ilizarov Fixation with Limited Open Reduction of Joint Surface and Distal Tibia Bridging Distraction of Ankle Joint
78: Two-Stage Treatment of a Chronic Foot Dislocation
84: Lapidus Fusion with External Fixation
65: Closed Correction of Club Foot with Ilizarov
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
