Fig. 1
(a) Clinical photos of the patient at the time of presentation to our clinic. (b) Note the soft tissue invagination into the underlying bone defect (green arrow). Patient presented after having a soft tissue flap and a static Ilizarov frame
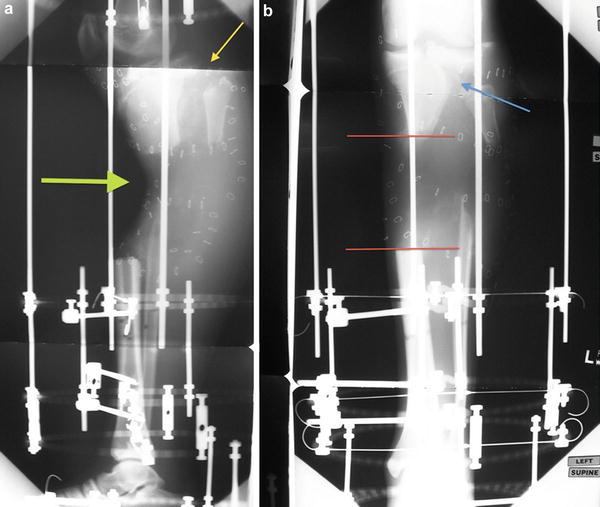
Fig. 2
(a) Lateral and (b) AP 36” pre-operative X-rays of the right tibia. Note the anterior translation of the distal segment, proximal tibia-fibular dislocation (yellow arrow). The XR also demonstrates the depression of the soft tissue (green arrow). (b) (red lines) Delineates the 9 cm proximal diaphyseal tibial bone defect . A lateral tibial plateau fracture with associated bone loss is also evident (blue arrow)
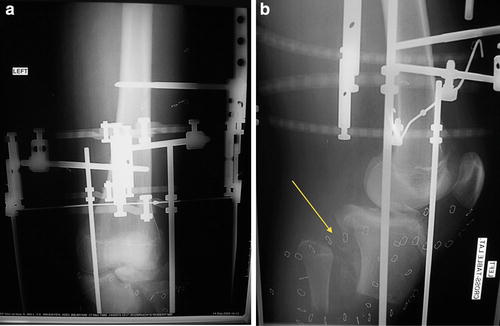
Fig. 3
(a) AP and (b) lateral XR of the knee. The knee-spanning Ilizarov frame was used to help maintain a reduced knee joint. Tibiofibular diastasis (yellow arrow) in addition to the lateral “shear”-type plateau fracture indicates the force vector during the initial trauma. These types of tibial plateau fractures are usually associated with knee dislocations
3 Preoperative Problem List
1.
s/p type IIIB tibial fracture with soft tissue coverage
2.
Soft tissue concavity into proximal tibial bony defect
3.
Nine cm proximal diaphyseal tibial bone defect
4.
s/p Ilizarov ring application, spanning the knee
5.
s/p ipsilateral knee dislocation
6.
Proximal tibiofibular dislocation
7.
Lateral tibial plateau fracture with metaphyseal bone loss
4 Treatment Strategy
This is a complex lower-extremity injury. Patient selection for limb salvage has been demonstrated to be related to a successful outcome. Motivated, educated patients with a good support system are best treated with this method. The soft tissue lesion was addressed with re-elevation of the flap and split thickness skin grafting. The lateral plateau and metaphyseal loss was addressed with Ilizarov wires. The proximal fibular fracture fragment was pulled into the defect using an olive wire. The bone defect was managed with two osteotomies and tandem transport. A knee-spanning Ilizarov frame with hinges for motion was utilized to treat the concomitant knee dislocation.
5 Basic Principles
1.
Be aware of knee dislocation fracture patterns. Stabilization of the knee is essential. The hinged construct allows joint ROM.
2.
Larger bone defects (>8 cm) require trifocal bone transport.
Related posts:
 8: Femoral Bone Defect
8: Femoral Bone Defect
 11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
 30: C3.3 Pilon Fracture Closed. Ilizarov Fixation with Limited Open Reduction of Joint Surface and Distal Tibia Bridging Distraction of Ankle Joint
30: C3.3 Pilon Fracture Closed. Ilizarov Fixation with Limited Open Reduction of Joint Surface and Distal Tibia Bridging Distraction of Ankle Joint
 78: Two-Stage Treatment of a Chronic Foot Dislocation
78: Two-Stage Treatment of a Chronic Foot Dislocation
 84: Lapidus Fusion with External Fixation
84: Lapidus Fusion with External Fixation
 65: Closed Correction of Club Foot with Ilizarov
65: Closed Correction of Club Foot with Ilizarov
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


