Fig. 1
Injury X-rays for Gustilo-Anderson Type IIIB open, severely contaminated tibia fracture with segmental bone loss

Fig. 2
Post-op initial irrigation and debridement and application of right ankle spanning external fixator

Fig. 3
X-rays post-irrigation and debridement, demonstrating bone loss
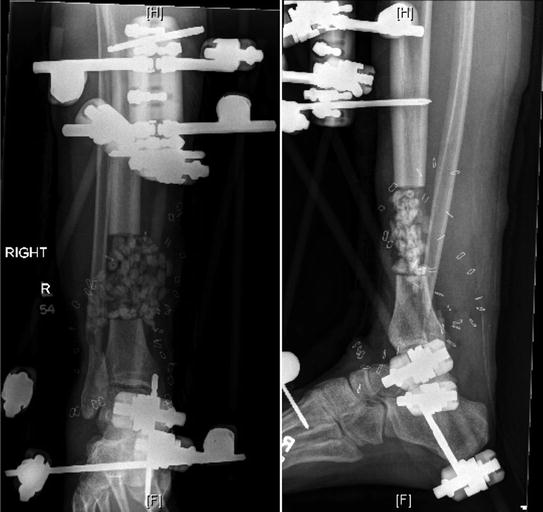
Fig. 4
X-rays post-operative tibial resection, placement of antibiotic-impregnated beads, and wound vacuum-assisted closure device application
3 Preoperative Problem List
1.
Grossly contaminated Gustilo-Anderson Type IIIB open pretibial wound requiring extensive soft tissue reconstruction
2.
Segmental tibial bone loss requiring bone transport
3.
Partial tibial nerve transection
4 Treatment Strategy
Given the gross wound contamination, extent of the soft tissue injury, and the partial tibial nerve transection, the patient received serial irrigation and debridements, by senior orthopedic and plastic surgeons, to delineate the extent of the injury and to ensure a clean wound prior to definitive treatment. The patient was treated with resection of all nonviable bone and tibial flat surface cuts were made for symmetry for future docking site surfaces. Antibiotic bead placement was used to fill the bone void following tibial resection and this provided local antibiotic delivery during serial irrigation and debridements (Fig. 4). Once a clean wound bed was achieved and soft tissue reconstruction was completed, tibial bone transport with an Ilizarov was planned for treatment of the tibial segmental bone defect. Ilizarov frame revision was planned once the docking site was approximated, to allow for compression across the docking site to stimulate union. Planned posterior iliac crest bone grafting of the docking site was discussed early with the patient and his wife. Lastly, a CT scan would be obtained once the docking site was approximated to ensure adequate healing, followed by Ilizarov frame dynamization. The regenerate should be monitored throughout treatment with dedicated X-rays focused on the regenerate site.
5 Basic Principles
Distraction osteogenesis is defined as the production of new bone between two vascularized surfaces created by an osteotomy and separated gradually by distraction. In 1989, Dr. Ilizarov described the Law of Tension-Stress, which states that “Gradual traction on living tissues creates stresses that can stimulate and maintain the regeneration and active growth of certain tissue structures… These regenerative processes depend upon the adequacy of the blood supply and the stimulating effect of weight bearing” (Ilizarov 1989a, b). There are four phases of treatment for distraction osteogenesis: corticotomy, latency, distraction, and consolidation. Bone transport is indicated for segmental bone defects, which may be the result of post-traumatic bone loss, chronic infection, bone resection for neoplasm, or treatment of atrophic nonunions. For distraction osteogenesis, a corticotomy close to the metaphysis is preferred, due to the increased blood supply, the greater trabecular surface area, and thinner cortices for the osteotomy, all of which promote healthy regenerate formation. The corticotomy should also be performed as atraumatically as possible, with care to maintain the periosteum (Delloye et al. 1990).
6 Images During Treatment
Related posts:
 8: Femoral Bone Defect
8: Femoral Bone Defect
 11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
 22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
 78: Two-Stage Treatment of a Chronic Foot Dislocation
78: Two-Stage Treatment of a Chronic Foot Dislocation
 84: Lapidus Fusion with External Fixation
84: Lapidus Fusion with External Fixation
 65: Closed Correction of Club Foot with Ilizarov
65: Closed Correction of Club Foot with Ilizarov
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


