, Paul N. Chugay1 and Melvin A. Shiffman2
(1)
Long Beach, CA, USA
(2)
Tustin, CA, USA
Abstract
The authors focus on the treatment of lateral thigh hypoplasia with discussion of the aesthetics of the ideal waist-to-hip ratio, the basic anatomy of the region, the preoperative marking of the patient, and the operative procedure. Postoperative care is described and potential postoperative complications are discussed with observed complications and the management of those complications. Fat grafting to the region is described and its impermanence versus silicone prosthesis placement.
Introduction
Over the course of time, what makes a woman beautiful and sexually attractive has changed. In the days of antiquity, a woman’s worth or beauty was largely attached to her ability to produce offspring. Since ovulation is not something that can be visualized by the naked eye, men have long used external cues to determine fecundity and health in females. Women with wider, “child-bearing” hips were noted to be more attractive. This fascination with the curvaceous female is well demonstrated in the art of the Baroque era. Peter Paul Rubens (1577–1640) was a German-born Flemish Baroque painter and a proponent of an extravagant Baroque style that emphasized movement, color, and sensuality. He was made famous for his love of portraying full-figured women that were curvaceous in their form, giving rise to the term “Rubenesque” when referring to plus-sized women. Over time, the concept of beauty changed from the more full-figured, curvaceous woman depicted by Rubens to an appreciation of the smaller figured, slender female [1]. Western cultures particularly began to idealize slimness and associated this with elegance, attractiveness, self-control, and youth. These women have been immortalized in the fashion magazines of the 1970s, 1980s, and 1990s. However, it seems of late that there has been a renewed interest in women with a more natural and curvaceous figure. Popular music and television icons such as Shakira, Jennifer Lopez, and Kim Kardashian have produced resurgence in the idea that the attractive woman has a more curvy appearance. A woman with a round bottom and curvy hips and thighs has again become sexy and a sign of true femininity. Although the amount of total fat that determines a maximally attractive female can vary from society to society and between time periods, it is clear that a curvy rather than straight female figure is still very important in identifying an attractive female form. For that reason, liposculpture has remained one of the top 5 most sought after cosmetic procedures among women, according to the American Society of Plastic Surgeons and the American Academy of Cosmetic Surgery [2, 3]. Liposculpture allows a surgeon to carve out a more pleasing figure even if the body mass index is not significantly changed. However, some women do not have the underlying boney and muscular structure to give them the desired curvy look or perhaps do not have sufficient fat to allow for lipo-contouring. To that end, hip implants have been introduced to help give women curves in the hip and lateral thigh area which could not have otherwise been created due to existing patient anatomy.
Waist-to-Hip Ratio
When discussing the curves that are deemed attractive in a female, one must have a discussion of the waist-to-hip ratio. The waist-to-hip ratio (WHR) is the ratio of the circumference of the waist to that of the hips. The World Health Organization (WHO) recommends that the waist circumference be measured at the midpoint between the lower margin of the last palpable rib and the top of the iliac crest. Hip circumference should be measured around the widest portion of the buttocks or at the level of the greater trochanter (Fig. 7.1) [4, 5].
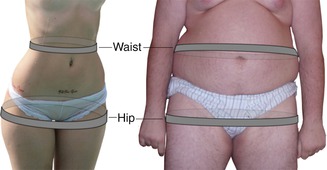
Fig. 7.1
Measurement of waist-to-hip ratio: in a lean person (left), the waist can be measured at its narrowest point, while for a person with a convex waist (right), it may be measured at about one inch above the navel. The hip is measured at its widest portion of the buttocks at left and at the greater trochanters at right
The WHR is frequently used as a measure of health risk as noted by the WHO and National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) [9]. A healthy WHR is between 0.67 and 0.80 in a healthy premenopausal woman and between 0.85 and 0.95 for a healthy adult male. The WHO and NIDDK have determined that a WHR above 0.95 in males and above 0.85 in females is associated with obesity and an increased risk of major diseases such as diabetes mellitus and coronary artery disease. Studies have found that women with a WHR of approximately 0.7 had optimal levels of estrogen and are less susceptible to diabetes, cardiovascular disorders, and ovarian cancers [6]. There has even been research that has found that the WHR was a more efficient predictor of mortality in older patients than waist circumference or body mass index [7]. Yusuf et al. [8], based on his evaluation of 27,000 participants, noted that if obesity were redefined using WHR instead of BMI that the proportion of people categorized as at risk of heart attack worldwide increases by threefold.
Along with being a method of assessing general health, the WHR has long been used as a measure of attractiveness. Due to hormonal changes during puberty, women preferentially deposit fat in the gluteofemoral region, while men tend to have an inhibition of fat deposition in the gluteofemoral region and deposit preferentially in the abdomen. This then gives women a low WHR closer to 0.7, while men typically have WHR closer to 0.9. As women age and fertility declines, skin laxity increases and the shape of the gluteal region usually changes as the content and distribution of fat and muscle change. The female hourglass shape fades and the waist-to-hip ratio approaches 1.0, similar to men, which in studies has been shown to give the female a less attractive score when evaluated by study participants [9]. Singh, an evolutionary psychologist, has argued in multiple articles since 1993 that the WHR is a significant measure of female attractiveness. Looking back at the women of ancient civilizations globally, female representations were most often in the range of a WHR of 0.6–0.7, suggesting a preference toward lower WHR in females. In the modern era, women who have a ratio near 0.7 are usually rated more attractive by men from European cultures [10]. Icons of the silver screen such as Marilyn Monroe and Sophia Loren, long touted as pinnacles of beauty, had a WHR close to 0.7 [10–12]. Singh [11] proposed a hypothesis to explain how WHR influences female attractiveness and its role in mate selection, citing evidence from studies of the WHR of Playboy playmates and Miss America winners over the past 30 years to support her work. Her hypothesis was plain and simple: regardless of time period or culture, a female with an hourglass figure as defined by the WHR near 0.7 was sexually attractive in practically all human societies. In a 2010 article, Platek and Singh [13] used functional magnetic resonance imaging (MRI) to demonstrate that male participants looking at naked female bodies with an ideal WHR (approx 0.7) showed excitation in the anterior cingulate cortex, an area associated with reward processing and decision making. To further evaluate the WHR as a signal of attractiveness, Dixson et al. [14] conducted a study using eye-tracking techniques to evaluate men’s fixation on digitally altered photographs of the same women. When asked to evaluate attractiveness, the men reliably chose women that had a larger breast size. However, regardless of breast size, women who had a WHR of 0.7 were rated as the most attractive. These studies all point to the premise that men appreciate curvy women and help us understand the change in modern culture toward the desire for a more shapely and voluptuous woman.
Women have gone to great lengths in the past to alter their WHR. The corset during the Victorian era (despite internal injuries caused to women) was popular as a tool to reduce a woman’s waist size to make her more physically attractive. Some women have resorted to hip and buttock padding to increase the apparent size of the hips and buttocks. Female cosmetic patients routinely employ liposculpture to help redefine their waist area. Of late, buttock augmentation with both fat and implants has been another means by which a woman can increase the curves in the lower pole of the body to help achieve a more aesthetically pleasing figure. Now, there is a way of providing a permanent solution for women who wish to increase their hip size to better suit the remainder of their figure and thereby alter their existing waist-to-hip ratio, potentially making them more attractive.
History of the Procedure
Based on a review of the literature, it seems that many physicians around the globe have been working concurrently in the past 2 years to produce a more aesthetic appearance to the hip/lateral thigh region using silicone prostheses [15–18].
The idea of reconstructing the thigh with a prosthesis was first introduced in 1995 by Kon et al. [19]. At that time, he published a paper explaining his experience with placement of a new type of implant for augmentation of the lateral thigh. A paraplegic patient was noted to have significant lateral thigh deficiency and was deemed a suitable candidate for reconstruction with a silicone prosthesis, measuring 29 × 7 cm. This implant was placed below the fascia lata. In 2005, Anger [20] presented his work on three patients who had medial thigh augmentation with calf implants for asymmetric medial thigh regions. He placed calf implants in the medial thigh via incisions made in the gluteal fold. The implants themselves were placed in a space that was dissected between the gracilis and adductor magnus muscles. Two patients received implants measuring 180 mL and a third patient received an implant with a volume of 140 mL. There were no complications noted and the results were satisfactory.
In 2011, several surgeons presented the results of their work over the preceding years, making it clear that thigh augmentation was definitely a surgery in evolution [16–18]. The first of the three studies to be published was our own institutions initial description of the procedure published in 2011 [18]. The authors evaluated the results of 18 hip augmentations since first beginning the procedure in 2010. In that paper the results were discussed with placement of a semirigid silicone prosthesis below the fascia lata via a lateral hip incision and noted only one significant complication: a case of suspected compartment syndrome. All 18 patients, however, had excellent aesthetic results and were happy with the procedure performed once recovery was complete. The implant used in our study was an oblong-shaped implant, designed by Nikolas Chugay, specifically for addition of volume and curvature to the lateral hip/thigh region (Fig. 7.2). In 2011, Netto [16] published his work on 68 patients who had placement of a silicone prosthesis in the lateral hip/thigh region. His work is a mix of patients being treated for poliomyelitis and those seeking more shapely thighs for purely aesthetic reasons. His paper also differs in the fact that the majority of his patients (94 %) had placement of medial thigh prostheses, and only four patients (6 %) had implants placed in the lateral aspect. Implants used in his procedures were of an elliptical shape, similar to those seen for calf augmentation. His implants varied in dimensions from 23 to 29 cm in length and 4–6 cm in width. His implants ranged in volume from 140 to 290 mL. In 2011 Cardak et al. [17] reported on his lateral thigh augmentation with a suprafascial approach to implant placement. The patient described was a 42-year-old female who had suffered a thigh deformity because of childhood orthopedic surgery, secondary to muscle atrophy and significant scarring. Similar to the work of Netto, Cardak used an asymmetrical silicone gel-filled calf prosthesis with more bulk at the cephalad aspect. His technique also used two incisions for placement of a 150 mL implant.
Fig. 7.2
Chugay hip prosthesis
Clearly, the field of thigh augmentation is in its infancy, and further long-term and large-volume studies are necessary to fully ascertain the long-term results, determine the best position for the implant, and assess the long-term ramifications of this surgery.
Indications
The hip implant, used in the authors’ practice, is designed to improve the aesthetic contour of the hip/lateral thigh region. First introduced as a means to correct a congenital anatomic deformity, the hip implant can be used to treat deformities due to trauma, disease, or after surgical procedures. Transgender patients are excellent candidates for hip augmentation to correct a naturally male form and produce more curvature in the lateral portion of the hip/thigh region. Asian women frequently lack fullness in the hips and do not have sufficient fat to perform a fat grafting procedure are excellent candidates for hip augmentation. Although a depression over the greater trochanter is natural, many females wish to accentuate this region and fill out the area to give them a more prominent curvature and benefit from the use of a hip implant.
Contraindications
A relative contraindication to placement of a hip implant would be a patient who is very thin and has little adipose tissue. This contraindication is relative only because it may allow for a palpable implant postoperatively, which is an often undesired complication of muscle augmentation surgery. Also, another relative contraindication would be previous surgery in the lateral hip/thigh region that may have compromised blood flow, as in major oncologic procedures or surgery after trauma. It is at the surgeon’s discretion to determine if a particular candidate can safely undergo surgery without major risk of compromise to tissues in the area.
Limitations
The surgeon is limited in the extent to which the lateral hip/thigh compartment can be augmented only by the implants currently available. Through work with our implant manufacturer, we have been able to create custom implants to augment larger segments of tissue. This, however, does come at an increased cost to the patient.
Relevant Anatomy
The anatomy in the lateral hip/thigh region that is encountered in the typical dissection is the area of relevant anatomy.
The tensor fascia lata (TFL) is a small muscle that lies in the middle and upper outer thigh. It arises from the anterior part of the outer lip of the iliac crest and inserts along the iliotibial tract at the middle third of the thigh. The tensor fascia lata then becomes continuous with the iliotibial band, which is a thick band of fascia that extends along the lateral thigh from the iliac crest to the knee (Fig. 7.3). The iliotibial band is inserted into the lateral condyle of the tibia (Gerdy’s tubercle). The tensor fascia lata assists in flexion and abduction of the thigh. It counteracts the posterior pull from the gluteus maximus muscle on the iliotibial tract. The innervation of the TFL is via the superior gluteal nerve which exits the pelvis at the greater sciatic foramen above the piriformis muscle [21]. It is below this muscle/band that the implant is placed snuggly against the femur to attain a seamless augmentation without high risk of implant palpability.
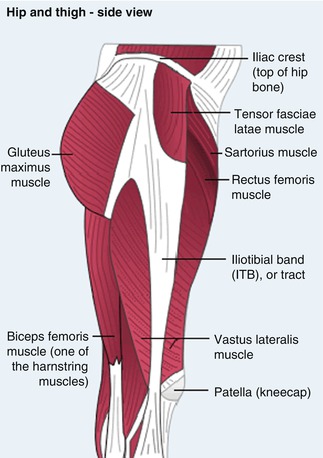
Fig. 7.3
Anatomy of the iliotibial band and tensor fascia lata
The nerve with the greatest potential for injury in this procedure is the lateral femoral cutaneous nerve of the thigh. It is a nerve of the lumbar plexus, arising from the dorsal branches of L2 and L3. The nerve exits the spine and courses anteriorly to cross under the inguinal ligament approximately 2 cm medial to the anterior superior iliac spine (ASIS). Once outside the pelvis, the nerve bifurcates into anterior and posterior branches approximately 5 cm below the ASIS on the surface of the sartorius muscle. The anterior branch becomes superficial about 10 cm below the inguinal ligament, and then it divides into branches that are distributed to the skin of the anterior and lateral parts of the knee. The posterior branch pierces the fascia lata and supplies the skin from the level of the greater trochanter to the middle of the thigh posteriorly [22]. The nerve is subject to injury at the time of dissection of the implant pocket below the fascia lata (Fig. 7.4).
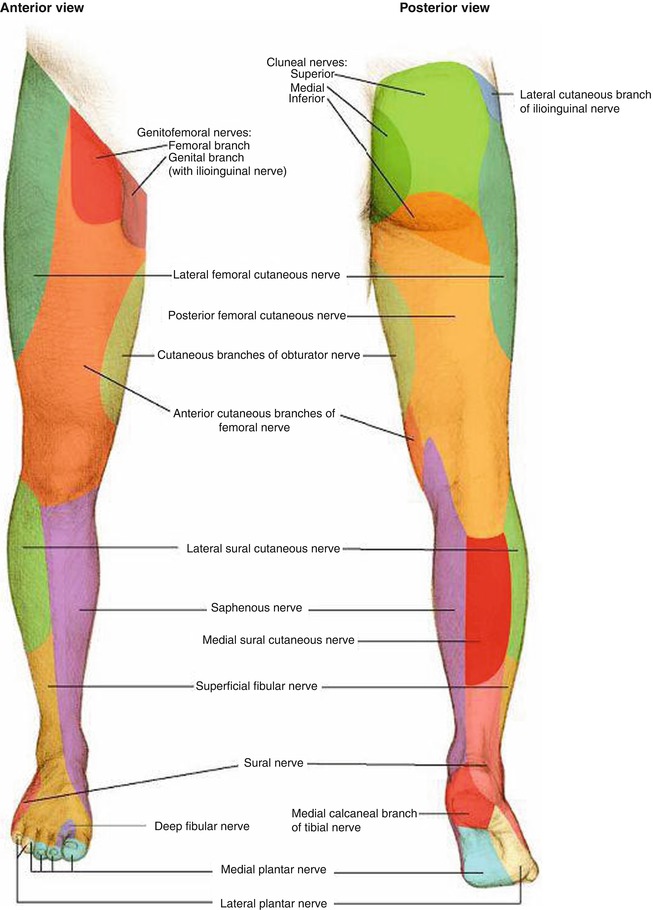
Fig. 7.4
Sensory dermatomes of the lower extremity. Take note of the dermatome relating to the lateral femoral cutaneous nerve as it is the most frequently involved in neuropathy post hip/thigh augmentation
Blood supply to the lateral hip/thigh region is primarily derived from branches of the femoral artery, of which the lateral circumflex femoral artery is the largest contributor (Fig. 7.5). This artery arises from the lateral side of the profunda femoris artery and passes horizontally behind the sartorius and rectus femoris, giving off three branches: ascending, transverse, and descending. The ascending branch then anastomoses with the superior gluteal and deep circumflex iliac artery to ensure a rich blood supply to the lateral hip/thigh region. These vessels are relatively remote from the area of dissection and are not at significant risk of injury if careful blunt dissection is performed and excessive medial dissection is avoided.
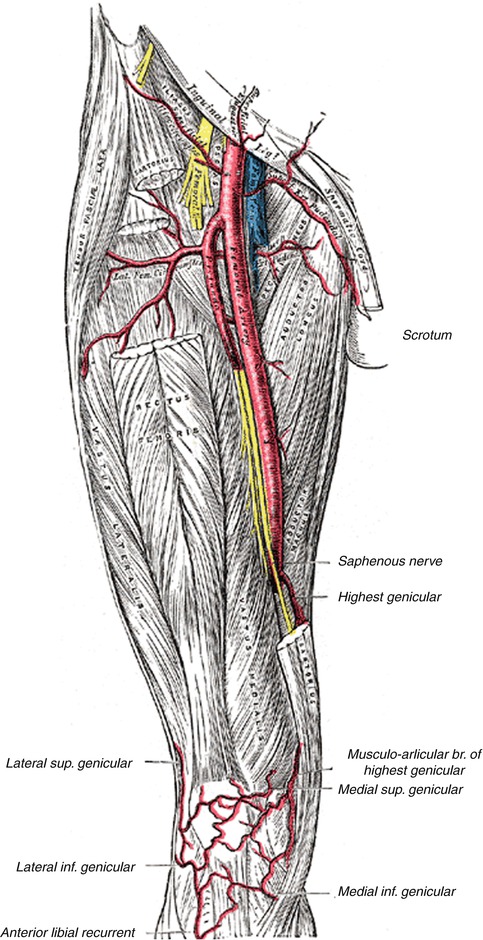
Fig. 7.5
Distribution of the femoral artery. Take note of the lateral branch of the femoral artery, the lateral femoral circumflex artery. It is this artery and its smaller branches that may be inadvertently damaged in the dissection of a pocket for the hip/thigh implant if one is not careful and dissection is carried too far medially
Consultation/Implant Selection
A thorough history and physical are paramount to preventing complications at the time of hip/thigh augmentation. During the consultation, patient’s expectations are managed and assessment of the patient’s mental state is undertaken. It is made clear to the patient the expected augmentation that can be seen with implant placement and limitations of the procedure are also explained.
After completion of the history portion of the consultation, an evaluation of the patient’s hip/thigh is made. Any asymmetries or defects are pointed out to the patient. The patient’s muscles are then evaluated. The skin and fat content are similarly assessed at this time as a patient with minimal adipose and thin skin is more at risk for implant palpability. Measurements of the patient’s thighs and hips are then taken: (1) circumference of the midportion of the thigh, (2) circumference of the waist, (3) circumference around the hips (level of the greater trochanters), and (4) length of the lateral leg from the greater trochanter to the mid-thigh (suspected insertion of the tensor fascia lata). Depending on the patient’s physical dimensions and desire for more volume in the lateral thigh regions, three different types of implants can be placed in the subfascial plane (small, medium, large). AART (Aesthetic and Reconstructive Technologies, Inc., Reno, NV) has been able to develop three different implants for the authors’ needs measuring 207, 250, and 545 mL (Table 7.1) (Fig. 7.6). The ability to place a larger implant is largely based on the length of the leg from the trochanter to the insertion of the tensor fascia lata, and implants should not be chosen that exceed this length.

Table 7.1
Hip implants with sizes, dimensions, and volume
Size | Catalog # | Width | Length | Projection | Size (cc) |
|---|---|---|---|---|---|
1 | 501–101 | 10.4 | 15.0 | 2.5 | 207 |
2 | 501–102 | 11.0 | 15.6 | 3.1 | 250 |
3 | 501–103 | 13.5 | 18.0 | 4.6 | 545 |
Fig. 7.6
Hip implant prior to implantation
Preoperative Planning and Marking
On the day of the surgery, the patient is met in the preoperative holding area. It is here that the patient’s consent is verified and again risks, benefits, and alternatives are reviewed with the patient. With the patient in the erect position, the proposed site of incision is marked, measuring approximately 5–7 cm. The site of incision should be in line with the patient’s bikini line/panty line so as to make the incision as well hidden postoperatively as possible (Fig. 7.7). Once the site of the incision is marked, the site of the proposed implant is marked taking into account the patient’s anatomy and existing deficit along with the desires of the patient.
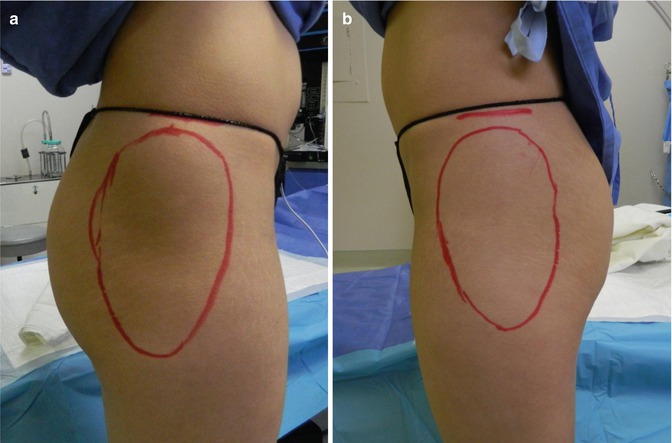
Fig. 7.7
(a, b) Preoperative markings with locations of incisions and proposed sites of implants
Operative Technique
A 3 cm incision is made in the high lateral aspect of the thigh in a transverse orientation, using a No. 15 Bard-Parker blade (Fig. 7.8). Dissection through the subcutaneous tissues is performed using both blunt and sharp dissection down to the level of the fascia (Fig. 7.9). A transverse incision is made in the fascia overlying the fascia lata muscle using a No. 15 blade (Fig. 7.10). This incision is lengthened using Metzenbaum scissors, and 2-0 Vicryl stay sutures are placed in the fascia lata on both sides (Fig. 7.11). A hemostat is used to divide the fascia lata muscle in line with its fibers. Dissection beneath the fascia lata is performed in a blunt fashion using finger dissection at first, taking care to achieve a level right on top of the femur (Fig. 7.12). A spatula dissector and a hockey-stick dissector are used to further expand the pocket to the edges of the pre-marked implant site just as in gluteal augmentation. Hemostasis is now assessed and attained as necessary with electrocautery. Once the pocket has been completed over the shaft of the femur, it is irrigated with a solution containing Betadine, normal saline, 1 g of cefazolin, and 80 mg of gentamicin. This is suctioned. 10 mL of 0.5 % Marcaine is instilled into the pocket to aid with postoperative pain control. A custom Chugay lateral thigh prosthesis is then placed (Fig. 7.13




Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
