THE BONY ORBIT AND THE PERIORBITAL
John L. Wobig and Roger A. Dailey
THE BONY ORBIT
The bony orbit consists not only of the smooth bony surface to which the soft tissues of the orbit are anchored but also of the structures within and adjacent to its orbital surface. What one might call the “adnexa” of the bony orbit means all of the nasal air sinuses, orbital fissures, anterior cranial and infratemporal fossal, and orbital foramina. Because these structures often require as much attention from the ophthalmologist as from the rhinologist and physicians in other specialties, the patient’s best interest demands that the ophthalmologist be equally as skilled in diagnosing abnormalities.
DEVELOPMENT
At the end of the first fetal month, the optic axes are positioned at an angle of ~ 160 degrees with reference to each other; at the end of the second fetal month, they are at an angle of ~ 80 degrees and, after the third month, at ~ 60 degrees, where they remain. In the adult, the medial orbital walls are roughly parallel and the lateral walls are approximately at right angles to each other.
The orbital cavities are large, four-sided, pyramidally shaped spaces. The base is forward and lateral and is outlined by the orbital margin. The apex, directed backward medially, is at the optic foramen.
In the adult male, the transverse diameters of the orbit are about 4 cm at the orbital margin, 3.5 cm high, and 4.5 cm deep, making the orbital rim wider than it is high (Fig. 14-1).
The orbit attains its full dimension from the fifth to the seventh year, or even later. Whitnall reported that adult orbital measurements are attained at puberty. Mann stated that the eye reaches adult measurements by the time the child is 9 years of age. Changes that may follow enucleation of the eyeball during the period of orbital growth emphasize the practical importance of this growth period. The orbit conforms to the law of adaptation of the organ to the function that it must fulfill. If the globe must be removed before the orbit has fully formed, orbital growth is checked.
THE ORBITAL MARGIN
The orbital margin is strong and not readily broken by injuries. The frontal bone forms it above, the zygomatic bone laterally, and the zygomatic and maxillary bones below. The sharp inferior margin continues medially and upward as the anterior lacrimal crest on the frontal process of the maxilla; here it forms the anterior boundary of the nasolacrimal canal and lacrimal fossa, at whose top it becomes indistinct. This is considered to be the medial part of the orbital margin. When one follows the superior margin downward on the medial side, however, one finds that the margin continues as the posterior lacrimal crest and connects with the anterior lacrimal crest at the lacrimal tubercle.
The supraorbital notch (75%) or foramen (25%) is found at the junction of the medial third and the lateral two-thirds of the supraorbital margin. It transmits the supraorbital vessels and nerves. A vertical line dropped from this notch strikes the infraorbital margin at a point behind which the inferior oblique muscle arises. This maneuver aids in locating the inferior oblique muscle during tenotomy. The infraorbital foramen is also in the vertical plane of the supraorbital notch. The notch serves as a surface landmark for block anesthesia of the supraorbital, frontal, and infraorbital nerves.

The four walls of the orbital cavity are (1) roof, or superior, or cerebral wall; (2) lateral, or outer, or temporal wall; (3) floor, or inferior, or maxillary wall; and (4) medial, or nasal, or ethmoidal wall.
THE ROOF
The roof is formed by the orbital portion of the frontal bone and the lesser wing of the sphenoid (Fig. 14-2). Its length is ~ 51 mm. It terminates medially at its junction with the lacrimal and ethmoidal bones and the orbital plate of the sphenoid.
This line of separation extends backward into the superior orbital fissure. The optic foramen lies just above this line. It is considered to form the apex of the roof. Laterally its boundaries are the superior orbital fissure and the frontosphenoidal and frontozygomatic structures.
Often the roof, divided into two tables medially and anteriorly, encloses extensions of the frontal and ethmoidal sinuses for a variable distance. Anteriorly, these sinuses may extend across the entire roof. Posteriorly, ethmoidal cells often invade the lesser wing of the sphenoid. The roof is arched from the front backward and from side to side, especially laterally and anteriorly in the region called the fossa of the lacrimal gland. Medial to the supraorbital notch and 4 mm behind the orbital margin is the fovea for the pulley of the superior oblique muscle.
THE LATERAL WALL
The lateral wall is the strongest orbital wall (Fig. 14-3). Its length and that of the medial wall are about the same (47 mm). Because the lateral wall is placed at an angle of ~ 45 degrees with the medial wall, the medial wall extends about 1 cm farther forward than the lateral. The zygomatic bone forms its anterior one-third and the orbital surface of the greater wing of the sphenoid its posterior two-thirds. The lateral angular process of the frontal bone completes it. The infraorbital fissure separates a considerable portion of the lateral wall from the floor, and the supraorbital fissure separates it from the roof.


The lateral wall also contains the zygomatico-orbital foramina, which lead into the zygomaticofacial and zygomaricotemporal canals that transmit the vessels and nerves of the same names. The anastomotic lacrimal branch of the zygomaticotemporal nerve leaves its canal through a foramen on the orbital surface of the lateral wall. It then unites with the lacrimal nerve and carries the parasympathetic fibers to the reflex lacrimal glands. About 10 mm below the zygomaticofrontal suture on the medial aspect of the bone is a small elevation, the lateral orbital tubercle. This marks the center of a larger area of attachment of soft tissues called the lateral ocular retinaculum, to be described later.
The supraorbital fissure communicates with the brain case and transmits the third, the fourth, the ophthalmic division of the fifth, and the sixth cranial nerves, the ophthalmic veins, a branch of the ophthalmic artery (or the orbital branch of the middle meningeal artery), and the sympathetic root of the ciliary ganglion. The spine of the lateral rectus muscle is about midway on the lower margin of the fissure.
The infraorbital fissure extends outward and laterally between the lateral and inferior walls. Posteriorly, it communicates with the pterygopalatine fossa; anteriorly, with the infratemporal fossa. It transmits the zygomatic branch of the maxillary division of the fifth nerve, the infraorbital nerve and vessels, and the venous communications between the inferior ophthalmic veins and the pterygoid plexus.
THE FLOOR
The floor of the orbit, formed by the zygomatic bone, the orbital surface of the maxilla, and the orbital process of the palatine bone, is the shortest wall, being two-thirds as deep as the others, and begins medially beneath the lamina papyracea. Its length is ~ 40 mm (Fig. 14-4). Like the other walls, its shape is roughly triangular. The orbital surface of the maxilla, which forms the greater part of the floor, presents the infraorbital groove that passes forward from the infraorbital fissure and becomes the infra-orbital canal.
The bone medial to the infraorbital grove and canal is the orbitoantral partition or orbital plate. It is the part most frequently involved in blow-out fractures. Posteriorly, the infraorbital fissure separates the floor from the lateral wall. Anteriorly, the floor is continuous with the lateral wall. The fossa of origin of the inferior oblique muscle is a roughened area that forms the anteromedial angle of the floor, just behind and lateral to the opening of the nasolacrimal canal (the relation of the anteromedial angle of the floor to the lacrimal fossa is discussed with the medial wall of the orbit).
THE MEDIAL WALL
The medial wall is nearly parallel with the mid-sagittal plane, although it bulges somewhat laterally (Fig. 14-5). It curves gradually into the inferior wall, particularly its posterior portion. Since it is formed by the frontal process of the superior maxilla, the orbital surface of the lacrimal bone, the lamina papyracea of the ethmoidal labyrinth, and a portion of the sphenoid bone, it is in direct relation to the lower part of the frontal, the ethmoid, and the sphenoid sinuses.

The openings into the anterior and posterior ethmoid canals are at the junction of the lamina papyracea and the orbital plate of the frontal bone. They transmit the ethmoidal vessels and nerves. Through the anterior ethmoid canal, the nasociliary nerve passes back into the cranial cavity, in the olfactory groove, where it again leaves through the ethmoid fissure to enter the nasal cavity as the anterior-internal nasal nerve. Anesthetics applied or injected in this area will anesthetize the upper anterior part of the nasal cavity.
The medial wall is the thinnest of the orbital walls. This point is important; accidental perforation of its superior part during exenteration may result in meningitis. That the medial wall often shows dehiscences in the paper plate of the ethmoid is of clinical interest because it may be responsible for orbital cellulitis secondary to ethmoiditis given that the mucous membrane of the ethmoid sinuses is in direct contact with the periorbita.

NASAL ANATOMY
The relationship of the medial orbital wall to the lateral wall of the nose is of great interest to the ophthalmologist. The lateral wall of the nose is composed of the nasal bone, the maxillary bone and its frontal process, the lacrimal bone, the labyrinth of the ethmoid and its two turbinates, the inferior turbinate, the perpendicular plate of the palatine, and the medial pterygoid plate of the sphenoid.
Inspection of the lateral wall of the nose from the anterior nares shows little more than the vestibule, the atrium of the middle meatus, and the inferior and middle conchae (turbinates). In a sagittal section (Fig. 14-6), one can see three conchae—inferior, middle, and superior—and the opened sphenoidal sinus. In addition to the atrium, one can observe the three meati—inferior, middle, and superior—as well as the olfactory groove and the sphenoethmoidal recess. The space between the lateral wall and the nasal septum, the common meatus, communicates with the other three meati and the sphenoethmoidal recess.
The sphenoid sinus opens into the sphenoethmoidal recess, the posterior ethmoid cells open into the superior meatus, and all of the rest of the sinuses open into the middle meatus. The nasolacrimal duct is the only opening into the inferior meatus.
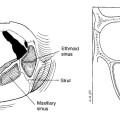
Removal of the middle turbinate reveals a remarkable area (Fig. 14-7). Anteriorly, a curved groove or gutter, the hiatus semilunaris, curves downward and backward. The uncinate process of the ethmoid bone forms its anteroinferior wall, and a bulging middle ethmoidal sinus, the bulla ethmoidalis, forms its superior border. One may think of the hiatus as the “spout” of a “funnel” open on its medial side. The top of the funnel, the frontal sinus, is connected to the hiatus by its intermediate part, the ethmoidal infundibulum. The anterior ethmoid sinuses and the maxillary sinus open into the hiatus; the middle ethmoid cells open above the bulla. A slight vertical bulging of the nasolacrimal canal may be present in front of the hiatus at the anterior end of the middle meatus.
Slightly above the posterior end of the attachment of the middle turbinate is the sphenopalatine foramen, which transmits the long and short sphenopalatine nerves from the sphenopalatine ganglion. Anesthetics applied to this area or injected through the foramen can affect the lacrimal parasympathetic nerves and the sphenopalatine ganglion.


Technically, the lacrimal fossa is not part of the orbital contents because it is outside the boundary set by the attachment of the septum orbitale. Its continuation, the nasolacrimal canal, is unquestionably an intranasal structure. The fossa seems to split the medial orbital margin in two. The upper part of the margin descends behind to form the posterior lacrimal crest; the lower part ascends anteriorly from the infraorbital margin to form the anterior lacrimal crest. The fossa is formed by the medial angular process of the frontal bone above, the lacrimal bone behind, and the frontal process of the maxilla in front.
The vertical lacrimomaxillary suture divides the fossa into two halves. When disarticulated, both the lacrimal and the maxillary parts have a curved surface called the sulcus lacrimalis or the “lacrimal groove.” As they descend in the articulated skull, they form the nasolacrimal canal, beginning at the point where the hamular process of the lacrimal bone articulates with the lacrimal notch, and ending ~ 12 mm below in the roof of the inferior meatus of the nose. The lacrimal process of the inferior concha assists in the formation of its medial wall.
The bone of the fossa anterior to the lacrimomaxillary suture is strong and solid, whereas the posterior part is thin, fragile, and invaded by anterior ethmoidal cells. Out of 100 dissections, Whitnall found that ethmoid cells extended “(i) to the posterior wall in 14 dissections, (ii) as far as the suture in the center in 32, and (iii) completely across the fossa in 54.”
In about 5% of surgical cases, we have found the anterosuperior angle of the maxillary sinus wedged in between the lower part of the tear sac and the frontal process of the maxilla. Removal of the anterior lacrimal crest in such a case will uncover the sinus mucosa medial to and above the lower part of the tear sac. In addition, the nasolacrimal canal and duct will be narrow and extend downward from the medial side of the broad but shortened tear sac, like the stem from the bowl of a tobacco pipe.
The upper end of the nasolacrimal canal forms the anteromedial angle of the orbital floor. Its lateral boundary is the incisura lacrimalis where the origin of the inferior oblique muscle is found. A tubercle, the spine of the anterior lacrimal crest, often marks this point. The anterior wall of the nasolacrimal canal is much thicker than the posterior wall. This can be demonstrated in tear sac surgery when the medial half of the canal wall is removed to expose the nasolacrimal duct.
Below, the canal opens at the highest point in the inferior meatus at the junction of the anterior one-third with the middle one-third of the inferior concha (turbinate). The opening of the nasolacrimal duct usually lies 5 mm or more beneath the bony opening. The medial wall of the nasolacrimal canal can often be seen in the nasal cavity as a vertical ridge descending from beneath the anterior attachment of the middle turbinate. This is important in intranasal tear sac surgery.
The anterior attachment of the septum orbitale is considered to be the limit of the orbital cavity; the lacrimal fossa and tear sac are, therefore, extraorbital. Just below the anterior lacrimal crest, there is a shallow sulcus, the sutura notha, in which a large nutrient foramen frequently exists. It may be related to the embryonic facial fissure. Often, in tear sac surgery, its margins are mistaken for the anterior lacrimal crest. Just behind the posterior lacrimal crest is the attachment of the medial ocular retinaculum.
THE PERIORBITA
The dura mater of the brain is composed of a meningeal layer and a periosteal layer. These two layers are so closely bound together that it is difficult to separate them. However, these layers separate after they pass through the optic foramen. The meningeal layer continues as the sheath of the optic nerve, and the periosteal layer lines the orbital fossa as the periorbita.
The periosteum through every opening in the orbit is continuous with the outer periosteum of the adjacent bones. It is continuous with the layer of dura mater at the supraorbital fissure and at the anterior and posterior ethmoidal cells. Traced through the orbital opening anteriorly, it is continuous with the periosteum of the bones of the face.
At the infraorbital fissure, the periosteal layer becomes the periosteum of the bones that form the infratemporal and pterygopalatine fossae. At the posterior lacrimal crest, the periorbita divides. The outer layer bridges over the lacrimal fossa where it is called the lateral lacrimal fascia. The inner layer, lining the bony wall of the lacrimal fossa, is continuous with the periosteum lining the nasolacrimal canal. The outer layer extends over the lateral surface of the lacrimal sac to which it is firmly adherent, and fuses at the anterior lacrimal crest with both the inner layer and the periosteum covering the anterior surface of the crest.
A projection from the union of the periorbita with the periosteum of the anterior surface of the facial bones forms the mesodermal layer of the embryonic folds of the upper and lower eyelids. Its marginal part later differentiates into the tarsus palpebrae and the rest into the septum orbitale in both eyelids. That part of the septum nearest the bony margins is the thicker, more resilient arcus marginale.
The periorbita is loosely attached to the walls of the orbit throughout most of its extent. It can be separated without difficulty except at the trochlear fossa, the lateral and medial ocular retinacula, the supraorbital and infraorbital fissures, and the optic foramen. Attached to its inner surface are numerous septal and fascial bands from various structures in the orbit.
A bundle of nonstriated muscle fibers, Müller’s orbital muscle, lies attached to the surface of the infraorbital groove. The fibers of this muscle completely fill the inferior orbital fissure and spread out “fan shaped” over the orbital floor. Posteriorly, they end beneath the annulus of Zinn. In humans, it represents the muscular sheet that completes the lateral wall of the orbit in other mammals, in which the bony wall is absent.
THE ORBITAL SENSORY NERVES
The orbital sensory nerves consist of the ophthalmic and maxillary divisions of the fifth cranial nerve that form at the anterior margin of the semilunar ganglion.
OPHTHALMIC DIVISION
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


